by Charlotte Kilpatrick | Oct 23, 2024 | Technology |
The National Institute for Health and Care Research (NIHR) announced in October 2024 that the first Phase III randomised trial of an investigational mRNA norovirus vaccine is opening across the UK. The trial seeks to evaluate the efficacy and safety of mRNA-1403 and is sponsored by Moderna. It will be conducted across 39 sites in the country, including 27 NHS primary and secondary care sites. Investigators hope to recruit 2,500 participants between late October and early 2025.
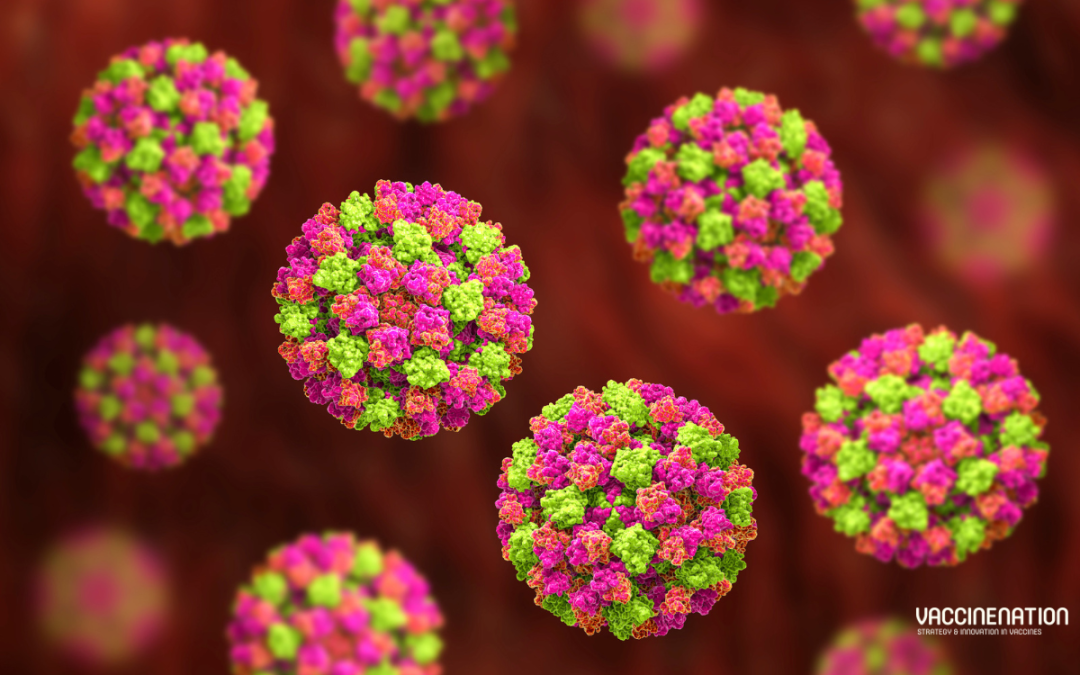
Norovirus
Norovirus, or the “winter vomiting bug”, is a viral illness; it is the “most common cause” of acute gastroenteritis globally. Symptoms include acute onset diarrhoea and vomiting, but there is evidence to suggest that norovirus infection is associated with intestinal inflammation and malnutrition and could cause long-term morbidity. WHO estimates that 685 million cases of norovirus are seen each year, including 200 million cases in children under 5.
“The burden of norovirus is significant; norovirus causes an estimated 200,000 deaths per year, including 50,000 child deaths, primarily impacting low-income countries. Norovirus has been estimated to cost $60 billion globally as a result of healthcare costs and economic losses.”
There are no licensed norovirus vaccines in use.
The trial
Participants in the trial will be randomly assigned to two groups. One group will receive the investigational vaccine, and the other groups will receive a placebo. While anyone who is aged 18 or older and meets the inclusion criteria is eligible for the trial, researchers are seeking participants aged 60 and older. This age group is “generally more likely to be severely affected by norovirus”. Thus, a successful vaccine would be of greatest benefit to them.
The trial is part of the 10-year partnership between Moderna and the UK Health Security Agency (UKHSA) on behalf of the UK Government. It is supported by the UK Vaccine Innovation Pathway (VIP) and the NIHR, which are working together to accelerate vaccine trials in the UK. The NIHR Research Delivery Network (RDN) is working with the devolved administrations to accelerate the roll-out of “key” vaccine studies. These efforts include the NIHR’s flagship recruitment tool: Be Part of Research.
Be Part of Research is an online service that connects people to health and care research across the UK. Anyone over the age of 18 can register for an account, indicating the areas of research that they are interested in. They are then sent information about suitable studies.
Advancing healthcare
The UK Chief Investigator, Dr Patrick, is a GP in Dorset and Research Director at the NIHR’s South West Regional Research Delivery Network. Dr Moore commented that the UK is “really pleased to be able to play an important role” in finding a vaccine for this “highly contagious disease”.
“Outbreaks of norovirus have huge consequences, both on our health systems and our economy. This innovative trial is crucial in helping us advance healthcare.”
NIHR Chief Executive and Chief Scientific Advisor to the Department of Health and Social Care, Professor Lucy Chappell, hopes that the vaccine could “make a difference to lives of many – especially our most vulnerable citizens”.
“Leveraging the UK’s expertise in vaccine development, the DHSC through the NIHR and Moderna are delivering this large-scale trial at pace, so that people across the UK and the world can benefit sooner.”
Health and Social Care Secretary Wes Streeting described the trial as a “huge vote of confidence in the UK’s life sciences sector”. It could also allow a “shift” away from sickness towards prevention, which would reduce pressure on the NHS and keep people healthier in the colder months. Moderna’s Chief Development Officer Dr Melanie Ivarsson is “delighted” to bring the trial to the UK.
“By advancing our investigational mRNA norovirus vaccine into a pivotal Phase III trial, we are one step closer to potentially providing a new tool to prevent infection from this highly contagious virus, which places a significant burden on health systems globally.”
Sarah Collins, Commercial Director at UKHSA, reflected that norovirus “isn’t just a nasty tummy bug – it can have serious consequences” including “disruption” to health services and education settings.
“It’s fantastic to see the first trial of its kind get underway as a result of UKHSA’s strategic 10-year partnership with Moderna, which aims to enhance investment in scientific research and vaccine development to enable a rapid response to future pandemics and other infectious diseases.”
For the latest on vaccine research, don’t forget to subscribe to our weekly newsletters here.
by Charlotte Kilpatrick | Sep 30, 2024 | Global Health |
In response to recent data on influenza-associated deaths in the United Kingdom and United States, experts from the UKHSA and the CDC are urging everyone who is eligible for a flu vaccine to get vaccinated. A survey from the National Foundation for Infectious Diseases (NFID) suggests that few adults in the United States intend to get vaccinated against flu, COVID-19, respiratory syncytial virus (RSV) or pneumococcal disease, expressing concerns about side effects and a “general distrust” of vaccines. A decrease in uptake has also been observed in the UK, a source of “real concern” for UKHSA.
NFID’s study
The National Foundation for Infectious Diseases (NFID) commissioned an annual survey of US adults to “better understand current attitudes and behaviours” about infectious diseases like influenza (flu) and COVID-19. The study was conducted in August 2024 and included 1,160 complete responses from adults aged 18 and over. The study found that, although 67% agreed that an annual flu vaccination is the “most effective” way of preventing flu-related hospitalisations and deaths, 45% did not plan to or were unsure if they would get vaccinated this season. Only 38% indicated intention to get a flu vaccine this year.
When asked about attitudes towards each disease, “less than 1 in 5” were concerned about themselves or someone in their family getting infected this season:
- RSV – 16%
- Flu – 17%
- Pneumococcal disease – 17%
- COVID-19 – 20%
The survey explored the “top reasons” for people who will or might get a flu vaccine to get vaccinated against flu, including:
- To protect yourself – 76%
- To protect your family – 65%
- To avoid severe complications, including hospitalisation and death – 51%
- To avoid getting sick and missing work or school – 51%
Nearly half (49%) of participants who are at higher risk for flu-related complications cited their chronic health condition as a reason to get vaccinated against flu. Almost 3 out of 4 (72%) of adults who were diagnosed with flu in the last 2 years were likely to get a flu vaccine.
Mistrust and confusion
The top reasons cited for not getting vaccinated included concerns about side effects and a lack of trust in vaccines. While 75% of respondents trust doctors, nurses, and pharmacists for information about vaccines, only 55% trust the CDC and 51% trust state and local health departments.
“Healthcare professionals remain the most trusted source of information about vaccines and play a critical role in protecting public health by providing clear, consistent, and strong vaccine recommendations.”
Data are concerning
At a press conference in September 2024, CDC Director Dr Mandy Cohen stated that in the previous flu season, “an estimated 25,000 people in the US died from flu or related complications”.
“We can protect ourselves and those we care about by getting updated vaccines to reduce the risk of serious illness from flu and COVID-19 and do more of the things we enjoy.”
CDC data indicate that the 2023-2024 flu season in the US was “moderately severe”, causing around 41 million illnesses, 490,000 hospitalisations, and 25,000 flu-related deaths. 199 children died due to flu-related illness, which matches the previous high from 2019-2020. Also at the press conference, Dr Robert H. Hopkins, Jr., NFID Medical Director, described vaccines as a “shield against illness” and an “important tool in our public health efforts”.
“The low vaccination rates among persons with chronic health conditions are of particular concern because they are more likely to develop serious and even life-threatening complications from respiratory infections.”
Dr Hopkins encouraged “everyone at increased risk” to speak to a healthcare professional about vaccination.
“Vaccines save lives, and we all play an important role in helping protect ourselves, our loved ones, and our communities from preventable infectious diseases.”
Dr Reed V. Tuckson, co-founder of the Black Coalition against COVID and chair of the board of the Coalition for Trust in Health & Science, emphasised the importance of building trust by “enhancing our support for people in using science and evidence to make personally appropriate decisions”.
“The pandemic taught us that it is possible to close some of the gaps in immunisation rates among communities of colour, but we still have a long way to go. In addition to evidence-based messaging, we know that guidance from familiar, trusted healthcare professionals working with minority communities is essential to building vaccine confidence.”
Similar concerns across the pond
UKHSA modelling suggests that in the 2023-2024 season, influenza-attributable mortality was around 2,776 deaths due to influenza, a significant decrease from 15,465 in the previous season. Estimates of influenza vaccine effectiveness (VE) against laboratory confirmed influenza in primary care ranged between 46% and 54%. Effectiveness against hospitalisation ranged from 30% in individuals aged 65 and above to 74% in children between 2 and 17 years. However, uptake was low in people with long-term health conditions (41%), 2- and 3-year-olds (44%), and pregnant women (1 in 3).
“Across eligible groups, influenza vaccine uptake in the UK was generally lower in the 2023 to 2024 season compared to the 2022 to 2023 season.”
The decrease from 2022-2023 to 2023-2024 is broken down into various risk categories:
- Aged 65 years and over: 77.8% compared with 79.9%
- Aged 6 months to under 65 years with one or more long-term health conditions: 41.4% compared with 49.1%
- Pregnant women: 32.1% compared with 35%
There was an increase observed in the 2- and 3-year-olds group, from 43.7% to 44.4%.
Get Winter Strong
A scaled-up Get Winter Strong campaign, the result of a collaboration between UKHSA, the Department for Health and Social Care, and NHS England, is set to launch on 7th October to “help reduce the impact of winter viruses on those most at risk” and ease NHS “winter pressures”. The campaign will urge people who are eligible to get their flu and COVID-19 vaccines when invited, and (for the first time) will encourage pregnant women to get RSV and whooping cough vaccination. The maternal RSV vaccine provides “strong protection” for newborns in their first few months of life, when they are at the greatest risk of severe illness from RSV.
Dr Gayatri Amirthalingam, UKHSA Deputy Director of Immunisation, emphasised that “getting vaccinated ahead of winter is by far your best defence” against the “many dangerous viruses circulating in our communities”.
“If you’re pregnant or have certain long-term health conditions, you are at greater risk of getting seriously ill. Older people and young infants with flu are also much more likely to get hospitalised. So, if you or your child are offered the flu, COVID-19, or RSV vaccines, don’t delay in getting them. Please speak to your nurse or doctor if you have any concerns.”
Maryam Sheiakh from Manchester is quoted by UKHSA reflecting on her experience with her daughter’s flu infection. Saffy, aged 4 at the time of infection, spent a week in hospital and was transferred to a High Dependency Unit. Luckily, Saffy made a full recovery, and Maryam encouraged parents to ensure that their children get vaccinated.
“Just go and get it, don’t take the risk. No parent wants to watch their child suffer like we did with Saffy.”
The Get Winter Strong campaign will last 10 weeks, appearing on television, radio, poster sites, and social media channels. What efforts are your national health agencies making to encourage vaccination ahead of the flu season, or how are they communicating the risks of infection and benefits of vaccination?
To discuss flu vaccine development and strategies with your colleagues at the Congress in Barcelona next month, get your tickets here, and don’t forget to subscribe to our weekly newsletters for the latest vaccine news.
by Charlotte Kilpatrick | Sep 27, 2024 | Global Health |
A study in The Lancet Public Health in September 2024 evaluates the measles dynamics in England between 2010 and 2019 to understand the effects of waning of vaccine-induced immunity. The researchers find that, although the MMR vaccine remains “highly protective” against measles infections for decades, and most transmission is “connected to people who are unvaccinated”, breakthrough infections in vaccinated individuals aged 15 years or older are “increasingly frequent”. However, they emphasise the importance of adequate coverage alongside vaccine effectiveness.
In England, measles “follows typical near-elimination transmission dynamics”, with “sporadic localised outbreaks and high national vaccine coverage”. England reached measles elimination status after “large outbreaks” between 2011 and 2013. From 2017 onwards a resurgence has been observed.
Highly protective vaccines
The authors describe measles vaccines as “highly protective against infection” recognising that they enabled a “great decrease in the global burden of measles” after immunisation programmes began in the 1970s and 1980s. Indeed, some countries became eligible for an elimination status since 2000 after the successful implementation of routine immunisation programmes. However, this is slipping out of reach for many countries in Europe and the Americas, which have reported a resurgence between 2015 and 2020.
“This resurgence was mostly reported in under-immunised communities and linked to past variations in vaccine coverage.”
Further outbreaks have been reported in “highly vaccinated” groups in Portugal and Japan, inviting questions about the waning of measles immunity in adults who had received two doses in childhood. Research suggests a waning of antibodies in young adults who had received two doses of vaccine “more than 20 years earlier”, in contrast to no decrease in previously infected individuals. Analysis of outbreak data suggest a “drop” in vaccine effectiveness in young adults who had received two doses of vaccine. However, effectiveness estimates appear to be “sensitive to assumptions on infection-induced immunity”.
The study
The study addressed the need to understand whether the measles case dynamics of settings with high vaccine coverage result from a waning of vaccine-induced immunity or if changes in the distribution of immunity in the population are driving the distribution of vaccine status among cases. A mathematical transmission model, stratified by age, region, and vaccine status was used to evaluate whether the measles dynamics in England from 2010 to 2019 were “in line with a waning of vaccine-induced immunity”. Three scenarios were modelled:
- Vaccinated individuals might only become infected because of primary vaccine failure
- Vaccinated individuals might become infected because of primary or secondary vaccine failure, with the risk of secondary vaccine failure depending on age
- Vaccinated individuals might become infected because of primary or secondary vaccine failure, with the risk of secondary vaccine failure depending on age and time since measles stopped being endemic
Each scenario was fitted to measles case data reported in England between 2010 and 2019, and the authors compared the resulting performance. Data were collected by UKHSA (formerly Public Health England), and included date of symptom onset, region of residence, age, and vaccine status. The final case dataset included 7,504 cases. The annual proportion of individuals who had been infected with measles and received two doses of the vaccine out of the overall number of individuals with measles was three times higher in 2019 than in 2011. The median age of individuals with measles was 12.5 years.
Results
Scenarios integrating waning of vaccine-induced immunity “better captured measles case dynamics” than the scenario without waning. In the scenario where waning started in 2000, the estimated waning rate was 0.039% per year.
“Although slow, waning was associated with an increased burden over time; setting the waning variable in this scenario to 0 led to a substantial decrease in cases.”
While overall vaccine effectiveness was estimated to stay high over the decades, the estimation suggested that the increasing number of breakthrough infections contributed to the measles burden in England. The additional burden brought by waning is “directly related to the risk of transmission from vaccinated cases”, as individuals infected by people who had been vaccinated would not have otherwise been infected.
“Our results suggest that the waning of vaccine-induced immunity likely explains the observed dynamics and age distribution of vaccinated measles cases in England between 2010 and 2019.”
Low vaccination rates a bigger factor
Dr Alexis Robert, Research Fellow in Infectious Disease Modelling at London School of Hygiene and Tropical Medicine (LSHTM) drew attention to the “biggest factor for measles outbreaks”: low vaccination rates. Dr Robert emphasised that the MMR vaccine is “highly effective” and two doses “will protect you and those around you”.
“This 0.04% waning each year is relatively slow, but because measles is so infectious, over time, this would add up to a ‘gap’ in a population’s defences the virus can exploit, which may increase the duration and size of outbreaks.”
The data patterns in the study emerge “because outbreaks have occurred as a result of declines in vaccine coverage”, said Dr Robert.
“If there were no outbreaks, this small amount of waning would not show up in any data. The key issue here is coverage, not the effectiveness of the vaccine.”
Dr Anne Suffel, co-author from LSHTM, agreed that the study “looks at one small part of the picture” and recognised that the “larger issue” is that “uptake of the MMR vaccine has been decreasing in England since 2015”.
“Understanding the impact of vaccine immunity waning will help anticipate the potential impact of measles in countries where incidence has been low for decades, but vaccine uptake is reducing. The best way to limit the impact of measles and protect everyone from what can be a horrible disease, is to keep vaccine uptake as high as possible.”
Dr Adam Kucharski, Professor of Infectious Disease Epidemiology and co-author from LSHTM, acknowledged the role of “other factors” such as “changes in testing patterns over time”.
“However, the consistency and age distribution of the increase in England – combined with reports of cases in vaccinated individuals in other countries and previous laboratory studies showing a decline in measles antibodies – suggests a biological explanation is involved.”
Join us at the Congress in Barcelona next month to explore the reasons for a resurgence in measles from an uptake perspective, and don’t forget to subscribe to our weekly newsletters for more vaccine news.
by Charlotte Kilpatrick | Sep 17, 2024 | Global Health |
A statistical report from UKHSA and NHS England in September 2024 reveals a drop in childhood vaccination coverage in England in 2023-2024. The report uses data from the COVER (cover of vaccination evaluated rapidly) programme, which collates information for children aged 1, 2, and 5 by financial year. The UK routine childhood immunisation programme includes WHO Europe’s recommendations as well as others advised by the Joint Committee on Vaccination and Immunisation (JCVI) and defined by UKHSA.
Coverage details
6-in1
For the 6-in-1 vaccine (previously 5-in-1), which protects against diphtheria, pertussis, tetanus, polio, disease caused by Haemophilus influenzae type b, and hepatitis B, vaccination is scheduled at ages 8, 12, and 16 weeks.
Coverage at 12 months in England has remained below the WHO Europe target of at least 95% of children immunised; for 2023-2024, 91.2% of children were reported to have completed their primary course of 3 doses at 12 months. This is a decrease from the previous year, which was 91.8%, and a continued “downward trend” since a peak of 94.7% in 2012-2013. In the 2023-2024 period, 8 out of 9 regions exceeded 90%, with 1 region (North East) exceeding the national target of 95%, reaching 95.2%. London had the lowest coverage of 86.2%.
Coverage at 24 months was 92.4%, lower than the previous year, which reached 92.6%, and continuing the “downward trend” since the peak at 96.3% in 2012-2013. This has not exceeded the target since 2018-2019. For regional coverage at 24 months, 8 out of 9 regions reached 90% coverage and 1 region met the national target of 95%. Again, London had the lowest regional coverage (87.7%).
At the 5-year coverage assessment, coverage was 92.6%, lower than the 93.2% coverage reported for the 5-in-1 vaccine in 2022-2023. This is the lowest since 2009-2009. However, at regional level, coverage exceeded 90% in 8 of 9 regions with the South West exceeding the 95% target. Once more, London had the lowest coverage (86.9%).
MMR
The MMR vaccine protects against measles, mumps, and rubella; doses are scheduled at 12 months (MMR1) and 3 years and 4 months (MMR2). Coverage is measured at 24 months (MMR1) and 5 years (both doses).
MMR1 coverage at 24 months reached 88.9% in 2023-2024; this is a decrease from 89.3% in the previous year and is the third consecutive year that coverage has been below 90%. For the 10 years between 2011-2012 and 2020-2021, coverage exceeded 90%. Regionally, 6 out of 9 regions reached 90% coverage, but no region met the national target of 95%. London had the lowest coverage (81.8%). At 5 years, MMR1 coverage was 91.9%, a decrease from 92.5% the previous year. 95% was achieved for the first and only time in 2016-2017; coverage has “consistently decreased” since then. The North East was the only region to meet the target of 95%.
MMR2 coverage at 5 years reached 83.9%, a decrease from 84.5% the previous year. Coverage decreased in all regions; no regions exceeded 90% coverage. The lowest coverage was in London (73.3%).
Rotavirus
The rotavirus vaccine is administered at 12 weeks and coverage is measured at 12 months; unlike other vaccines in the primary schedule, the rotavirus vaccine cannot be given beyond 6 months. This means that coverage at 12 months is “likely to be lower” than other vaccines.
National coverage at 12 months was 88.5%, a decrease from 88.7% in the previous year. This means that rotavirus vaccine coverage is “now at its lowest level since data became available” in 2016-2017. In 4 regions, coverage exceeded 90%, but none achieved 95%. London was the region with the lowest coverage at 83.6%.
PCV
The pneumococcal conjugate vaccine (PCV) protects against pneumococcal disease. The primary course is scheduled at 12 weeks and the booster dose at 12 months; coverage is measured at 12 months and 24 months.
The primary course coverage at 12 months was 93.2%, a decrease of 0.5% from 2022-2023. The booster coverage reached 88.2%, a decrease from 88.5% the previous year and a continuation of the downward trend since it peaks in 92.5% in 2012-2013. 5 out of 9 regions reached 90% coverage for the booster, but no regions exceeded the national target of 95%. London had “consistently lower coverage” between 2021-2024 and achieved 80.4% in 2023-2024.
Hib/MenC
The Hib/MenC vaccine protects against Haemophilus influenzae type b (Hib) and meningococcal disease group C (MenC). The combined vaccine is administered at 12 months, with coverage measured at 24 months and 5 years. It includes a booster for Hib, which is offered within the DTaP/IPV/Hib/HepB primary course.
At 24 months, coverage in England remained below 90% for the third year; it has declined consistently since a peak of 92.7% in 2012-2013. 88.6% of children were reported as having received the Hib/MenC vaccine. 6 out of 9 regions reached 90% coverage and no region achieved 95%. The lowest coverage was 81.2% in London. At 5 years, coverage was 89.4%, a decrease from 90.4% the previous year. This takes coverage to its lowest point since 2011-2012. 7 out of 9 regions reached 90% but no regions met 95%. London had the lowest coverage at 82.5%.
MenB vaccine and booster
The MenB vaccine and booster protects against meningococcal disease (group b). It is a combined vaccine scheduled at 8 weeks with a booster at 12 months, and coverage is measured at 12 months and 24 months.
At 12 months, 90.6% received 2 doses; this is a decrease from 91.0% the previous year. London had the lowest coverage at 85.5%. At 24 months, coverage was 87.3%, a decrease from 87.6% the previous year. Again, London had the lowest coverage (79.3%).
Parents encouraged to seek vaccines
Responding the report, Minister for Public Health and Prevention Andrew Gwynne urged parents to “take up vaccinations to keep children safe”, particularly as they return to school or nursery this Autumn.
“Vaccines are our best form of protection against serious illness.”
Steve Russell, NHS National Director for Vaccinations and Screening is concerned that “too many children are still not fully vaccinated” against vaccine-preventable diseases that can cause “serious illness”.
“Vaccinations have been protecting children for decades and are offered free as part of the NHS routine immunisation programme, saving thousands of lives and preventing tens of thousands of hospital admissions every year.”
UKHSA Consultant Epidemiologist Dr Vanessa Saliba emphasised the importance of the drive to increase vaccine uptake so that “no child is left at risk of serious illness or life-long complications”.
“These vaccines offer the best protection as children start their journey into nursery and mixing more widely. Many who missed out on their vaccinations have already been caught up, but more needs to be done to ensure all those eligible are vaccinated.”
For more on ensuring uptake levels match the pace of vaccine innovation, join us at the Congress in Barcelona next month. Don’t forget to subscribe to our weekly newsletters for the latest vaccine updates.
by Charlotte Kilpatrick | Aug 16, 2024 | Infection |
Data from the UK Health Security Agency (UKHSA) shared in August 2024 reveals a “concerning rise” in antibiotic-resistant gonorrhoea infections in England. In 2023 over 85,000 gonorrhoea diagnoses were reported in England; this is the highest number since records began in 1918. There were also 15 confirmed cases of infection with ceftriaxone-resistant Neisseria gonorrhoeae detected in England between June 2022 and May 2024. Since the initial case detected in England in 2015, there have been a total of 31 ceftriaxone-resistant Neisseria gonorrhoeae cases. UKHSA highlights the importance of “regular” STI testing, particularly for people who have “condomless sex with new or casual partners”.
Developing resistance
Gonorrhoea is the second most commonly diagnosed sexually transmitted infection (STI) in England. In 2023 the highest annual number of diagnoses (85,223) since records began was reported. The bacteria, Neisseria gonorrhoeae, has developed resistance to every class of antibiotics used to treat it. Cephalosporins are the last remaining class of antibiotics available for use as empirical monotherapy. The recommended first-line therapy is 1g ceftriaxone (a cephalosporin), but there are “sporadic” cases of infection with ceftriaxone-resistant N. gonorrhoeae.
16 cases were reported between 2015 and May 2022; since then, a further 15 ceftriaxone-resistant infections have been detected in England. Five of these recent cases were extensively drug-resistant (XDR). All 31 cases detected in England have been among heterosexual individuals, mostly in their 20s, and “most” have acquired infection in the Asia-Pacific region, which is the region with the highest prevalence of ceftriaxone-resistance.
UKHSA response
UKHSA has sent a clinical alert to sexual health services to “reinforce the need” to culture gonococcal isolates, perform test-of-cure, and refer all ceftriaxone-resistant N. gonorrhoeae strains or potential treatment failures to UKHSA. It also emphasises the importance of correct and consistent condom use to the public.
Dr Helen Fifer, Consultant Microbiologist at UKHSA, highlighted a concern that gonorrhoea could become “untreatable” in the future.
“Untreated gonorrhoea can lead to serious health issues, including pelvic inflammatory disease and infertility. Condoms are the best defence, but if you didn’t use one with a recent new or casual partner, get tested to detect the infection and prevent onwards transmission.”
Professor Matt Phillips, President of the British Association for Sexual Health and HIV (BASHH) described the rise of these antibiotic-resistant infections as a “worrying trend” that “must be addressed with immediate action”.
“Antibiotic resistance of STIs poses an increasingly major public health threat, which can create physical and psychological harms and place additional demands on other parts of the NHS.”
Professor Phillips stated that BASHH and sector partners have “repeatedly called” for a sexual health strategy for England.
“This must be a priority if our expert sexual health workforce are to effectively meet these growing and changing needs in sexual health.”
In January 2024 CARB-X announced funding for Intravacc’s vaccine efforts against gonorrhoea, which you can read about here. We also look forward to further exploring the role of vaccines in addressing the growing challenge of N. gonorrhoeae at the Congress in Barcelona this October, so get your tickets to join us there, and don’t forget to subscribe to our weekly newsletters here.
by Charlotte Kilpatrick | Aug 9, 2024 | Infection |
Data from the UK Health Security Agency (UKHSA) released in August 2024 reveal that 10,493 laboratory confirmed cases of pertussis in England were reported between January and June 2024. This compares with 856 laboratory confirmed cases reported in 2023. Since the outbreak began in November 2023, there have been 10 reported infant deaths; 9 of these deaths were reported between January and June 2024. UKHSA continues to urge pregnant women to get vaccinated to “protect their babies from birth onwards”.
Cases “notably high”
The last major outbreak of pertussis was recorded in 2012, followed by a cyclical increase in 2016; it is a cyclical disease that peaks every 3 to 5 years. Pertussis activity was “exceptionally low” in England between April 2020 to Summer 2023. Although numbers in 2023 “remained lower than pre-pandemic years”, an increase has since been observed in all age groups and in “every region” in England.
10,493 cases were confirmed between January and June 2024. Around half of these cases (5,769) were in people aged 15 years or older; 2,226 cases were reported in children aged 10 to 14 years and 1,253 cases in children aged 5 to 9 years. 328 cases were reported in infants younger than 3 months. These infants are at highest risk of severe disease and are too young to be fully vaccinated.
Vaccination in pregnancy
Although vaccination in pregnancy is “key to passively protecting babies” before they are “directly protected” through the infant vaccine programme, maternal vaccine uptake is declining. Uptake fell from 74.7% in December 2017 to 58.9% in March 2024. Pertussis vaccination is recommended in every pregnancy and is often administered around the time of the mid-pregnancy scan. To give maximum protection, the vaccine should be given before 32 weeks.
Dr Mary Ramsay, UKHSA’s Director of Immunisation, emphasises that vaccination is the “best defence against whooping cough”.
“It is vital that pregnant women and young infants receive their vaccines at the right time.”
As cases continue to rise and infant deaths are recorded, Dr Ramsay states that “ensuring women are vaccinated in pregnancy has never been more important”.
“Our thoughts and condolences are with those families who have so tragically lost their baby.”
The team at UKHSA return to the Congress in Barcelona to share their insights with the community in October, so do get your tickets to join these discussions and don’t forget to subscribe for weekly vaccine updates.
by Charlotte Kilpatrick | Jul 17, 2024 | Global Health |
The UK Department of Health and Social Care announced in July 2024 that the UK will become the first country in the world to offer a national vaccination programme with the same vaccine for the protection of infants and older adults from Respiratory Syncytial Virus (RSV). Based on advice from the Joint Committee on Vaccination, the Pfizer vaccine will be offered from August in Scotland and September in England, Wales, and Northern Ireland. The rollout includes a vaccine for pregnant women over 28 weeks, a routine programme for people over 75, and a one-off campaign for those aged 75 to 79.
A “relatively unknown” threat
Although RSV is “relatively unknown” to the public, it infects around 90% of children in the first two years of life. It typically causes mild, cold-like symptoms but can also lead to severe lung infections like pneumonia and infant bronchiolitis. It is a “leading cause” of infant mortality globally. Every year in the UK, RSV accounts for approximately 30,000 hospitalisations in children under 5 and between 20 and 30 infant deaths. It also causes around 9,000 hospital admissions in people over the age of 75.
RSV puts pressure on health services, so it is hoped that this programme could “free up thousands of hospital bed days” and prevent “hundreds of deaths” each year. This will be particularly important during “challenging winter months”. Minister for Public Health and Prevention, Andrew Gwynne, expects that the vaccine will “save lives and protect the most vulnerable” but also “ease pressure on our broken NHS”. Gwynne reflected on his own experience with the “devastating effects” of the disease.
“My own grandson contracted RSV when he was just days old, leading to weeks in intensive care, and a lifelong impact on his health. I don’t want anyone to go through what he went through.”
A “huge step forward”
Steve Russell, NHS national director for vaccinations and screening, emphasised that RSV is a “very serious illness”.
“This rollout is a huge step forward and will undoubtedly save the lives of many of those most at risk.”
Russell “strongly” encourages people aged 75 to 79 to come forward for vaccination when they are invited, and for women who are 28 or more weeks pregnant to contact their maternity service or GP surgery to “ensure their baby is protected”. Professor Dame Jenny Harries, UKHSA Chief Executive, stated that the vaccine “offers huge opportunities to prevent severe illness in those most vulnerable to RSV”. This will “protect lives and ease winter pressures for the NHS”.
“UKHSA has provided critical scientific information to evidence the benefits of a national RSV immunisation programme and so the rollout of the vaccine is a truly positive moment for the public’s health.”
Will the procurement of an “effective vaccine” and a programme to protect both infants and older people, UKHSA is “working rapidly” with the NHS and Local Authority colleagues to prepare for September.
“Please do come forward if you are eligible.”
RSV remains a priority theme on the Congress agenda this October, so do join us to contribute to discussions, and don’t forget to subscribe to our newsletters for more vaccine updates.
by Charlotte Kilpatrick | Jul 11, 2024 | Infection |
In July 2024 the UKHSA shared data revealing that cases of whooping cough are still increasing with 2,591 cases confirmed in May. A significant number of these cases are reported in babies under 3 months old, who are at greatest risk from the infection. Sadly, there have been 8 infant deaths already this year. UKHSA urges vaccination in pregnancy to protect against infant death.
Cases on the rise this year
In England, 7,599 laboratory confirmed cases of pertussis were reported to UKHSA between January and May 2024. Case numbers have been increasing each month: 555 in January, 920 in February, 1,427 in March, 2,106 in April, and 2,591 in May. In this time there have also been 8 reported infant deaths. Of the total cases between January and May 2024, around half (53.4%) were in patients aged 15 years or older and 23.0% were in children between the ages of 10 and 14 years.
The number of confirmed cases in infants under 3 months, the age group most at risk of severe disease and too young to be fully vaccinated, reached a high of 407 in the 2012 outbreak. Between January and May 2024 there were 262 infants under 3 months with confirmed pertussis.
The increase, observed since December 2023, is attributed to a “combination of factors”. Whooping cough is a cyclical disease with peaks every 3 to 5 years; the last cyclical increase occurred in 2016. During the COVID-19 pandemic, restrictions and public behaviours drove case numbers down. A peak year is therefore “overdue”.
Vaccination during pregnancy
Young children are at highest risk of severe complications and death, but vaccination at the “right time” in pregnancy is “highly effective”, providing 92% protection against infant death. However, vaccination in pregnancy uptake data reveal a continued decline; coverage in March 2024 was 58.9% compared to the peak coverage of 72.6% in March 2017.
Dr Mary Ramsay, UKHSA Director of Immunisation, describes vaccination as the “best defence against whooping cough”.
“It is vital that pregnant women and young infants receive their vaccines at the right time. Pregnant women are offered a whooping cough vaccine in every pregnancy, ideally between 20 and 32 weeks.”
Vaccination in pregnancy “passes protection” to the baby for the first months of life when they are “most vulnerable” and too young for their own vaccines. Dr Ramsay offered “thoughts and condolences” to the families who have “so tragically lost their baby” in the outbreak and emphasised the importance of “ensuring women are vaccinated appropriately in pregnancy”. England’s Chief Midwifery Officer, Kate Brintworth, shared “real concern” at the rise in cases and deaths.
“I would urge pregnant women to get vaccinated to help protect their babies in the first few weeks of their life. You can speak with your GP or maternity team if you have any questions about the vaccine.”
Brintworth stated that the NHS is continuing to “identify areas at greater risk” and respond with “robust local vaccination offers”.
“Women can access the vaccine, which also protects against diphtheria and tetanus, through their GP or some antenatal services, and parents should also ensure that their children get protected in the first few months after birth as part of the routine NHS vaccine offer.”
For more from senior representatives of UKHSA at the Congress in Barcelona, get your tickets to join us, and don’t forget to subscribe to get weekly vaccine updates here.
by Charlotte Kilpatrick | May 20, 2024 | Infection |
The UKHSA shared guidance and information on cryptosporidium in May 2024 following South West Water’s acknowledgement that “small traces” of the parasite were identified in Brixham, south Devon. The water company is investigating the source of the outbreak, with 46 cases of cryptosporidiosis already confirmed. The company issued a boil water notice to residents as 46 confirmed cases were reported and over 100 people contacted their GPs about symptoms. The “microscopic” parasite causes cryptosporidiosis, which is “unpleasant” and “sometimes dangerous”.
What is cryptosporidium?
Cryptosporidium is a “nasty bug” that resides in the intestines of infected humans and animals. It is passed out in poo, when it can spread and contaminate water sources and food. It causes cryptosporidiosis, which is particularly common in young children, people who work with farm animals and contaminated waters, people changing nappies, and those who travel to countries with “poor sanitation”. It can cause “serious illness” in people with weakened immune systems.
Symptoms are “deeply unpleasant”, including severe watery diarrhoea, vomiting, stomach cramps, nausea, fever, or loss of appetite. It can last around 2 weeks. Prevention relies on “simple hygiene” steps, as there is no vaccine:
“The development of partial immunity after exposure suggests the possibility of a successful and effective vaccine, but protective surrogates are not precise.”
There is also no treatment, but rehydration is recommended after diarrhoea.
Outbreak in Devon
In May 2024 the BBC reported that South West Water (SWW) had suggested that a “faulty valve” may have created a route for the parasite into the water network. Laura Flowerdew, chief customer officer emphasised that the team is “doing further work to make sure we’re absolutely confident that’s the cause and the only cause”.
“We’re working through operational procedures in the meantime…public health is our absolute priority at this point.”
However, Anthony Mangall, MP for Totnes and South Devon, was “very concerned” with the response to the outbreak, suggesting that they had been “slow to act” and displayed “poor” communication with customers.
Expert opinion
Professor Paul Hunter from the University of East Anglia (UEA) commented that “in people with severely weakened immune systems it can cause severe disease and can even be fatal”. He suggested that “before effective antiretroviral treatments” for HIV/AIDS, cryptosporidium could be “fatal as recovery didn’t happen”.
“With effective control of AIDS nowadays we see far less severe cryptosporidiosis. There is no effective drug treatment for cryptosporidiosis and all we can do is keep people comfortable and replace fluids until recovery happens.”
Professor Hunter believes that there are “far fewer outbreaks now” than in the 1990s when he was “more involved” thanks to “improvements in treatment plants”. However, without regular summaries from UKHSA it is hard to know how many outbreaks have occurred.
For more on infectious disease outbreaks and control, why not subscribe to our weekly newsletters here?
by Charlotte Kilpatrick | May 17, 2024 | Global Health |
In May 2024 the UK Government announced that it will commit up to £85 million to the “growing threat” of antimicrobial resistance (AMR). At an event hosted by the Royal Society, global leaders came together to agree actions for tackling AMR and to hear accounts from AMR survivors. In the same week, WHO released the updated Bacterial Priority Pathogens List (BPPL) 2024, which features 15 families of antibiotic-resistant bacteria for prioritisation.
UK investments
The following initiatives were announced by the government:
- Up to £50 million to partner with countries in Africa to improve access to essential antimicrobial drugs, building on work by the UK Global AMR Innovation Fund and local expertise.
- Up to £25 million including partnering with countries and territories in the Caribbean to strengthen AMR surveillance systems and enable accurate monitoring of threats, through regional partners such as the Caribbean Public Health Agency and PAHO. This builds on the existing investment in the Fleming Centre in London and will allow the government to explore how to support the delivery of AMR centres in alignment with the Fleming Initiative.
- Up to £10 million over 5 years to help establish a global independent scientific panel for AMR, modelled on the success of other international panels such as the Intergovernmental Panel on Climate Change (IPCC).
- Alongside these programmes, £1.8 million has been allocated to the creation of a dedicated team in MHRA to support creating novel antimicrobials and diagnostics.
The projects “build on ongoing international and domestic work” to prevent the spread of AMR. Health Minister Andrew Stephenson commented that AMR is a “threat the world must take extremely seriously” and could “render our most vital medicines useless”. UKHSA reports that in 2019 4.95 million global deaths were associated with drug-resistant bacterial infections. By 2050 this is set to rise to 10 million, and the global economic cost of this is calculated to be $100 trillion.
The Foreign Secretary, Lord Cameron, identified AMR as a “global emergency posing a vast threat to our health, our development, and our security”.
“We must do more to tackle this threat and do it together, because it is too big to tackle without united global action.”
Jeremy Hunt, Chancellor of the Exchequer, is “deeply concerned” about the threat AMR poses “not just to the UK but to the world”.
‘The COVID-19 pandemic was conclusive proof that health emergencies don’t respect borders. That’s why I’m proud that the UK continues to play a pivotal role in bringing countries together to tackle emerging global health threats.”
UK Special Envoy on AMR, Dame Sally Davies, suggested that the “emergency is an existential threat to communities everywhere”. Dame Davies was “honoured” to host the event, which “represents a pivotal milestone for the world to move forward together and play a part in safeguarding our antibiotics for generations to come”.
“I call on everyone to join us to make equity, One Health, and action the cornerstone of our next steps to tackle AMR.”
Dr Colin Brown, Deputy Director of Clinical and Emerging Infections at UKHSA, is concerned that “simple lifesaving interventions in the form of antimicrobials are in danger of becoming ineffective”.
“Tackling the issue is a priority for UKHSA but long-term success requires global action. For antimicrobials to remain available and work effectively for everyone, we need international surveillance to identify new areas of AMR and collaboration. We also need to ensure expertise is being shared to help uncover new approaches to therapies and diagnostics for treating drug-resistant diseases.”
WHO’s BPPL
WHO’s updated BPPL “incorporates new evidence and expert insights” to inform R&D for new antibiotics and “promote international coordination to foster innovation”. Dr Yukiko Nakatani, WHO’s Assistant Director-General for Antimicrobial Resistance ad interim, believes the list is “key” to “guiding investment and grappling with the antibiotics pipeline and access crisis”.
“Since the first Bacterial Priority Pathogens List was released in 2017, the threat of antimicrobial resistance has intensified, eroding the efficacy of numerous antibiotics and putting many of the gains of modern medicine at risk.”
Dr Jérôme Salomon, WHO’s Assistant Director-General for Universal Health Coverage, Communicable and Noncommunicable Diseases, stated that AMR “jeopardises our ability to effectively treat high burden infections”, which leads to “severe illness and increased mortality rates”.
The list
Critical priority:
- Acinetobacter baumannii, carbapenem-resistant;
- Enterobacterales, third-generation cephalosporin-resistant; and
- Enterobacterales, carbapenem-resistant;
- Mycobacterium tuberculosis, rifampicin-resistant (included after an independent analysis with parallel tailored criteria, and subsequent application of an adapted multi-criteria decision analysis matrix).
High priority:
- Salmonella Typhi, fluoroquinolone-resistant
- Shigella spp., fluoroquinolone-resistant
- Enterococcus faecium, vancomycin-resistant
- Pseudomonas aeruginosa, carbapenem-resistant
- Non-typhoidal Salmonella, fluoroquinolone-resistant
- Neisseria gonorrhoeae, third-generation cephalosporin- and/or fluoroquinolone-resistant
- Staphylococcus aureus, methicillin-resistant
Medium priority:
- Group A streptococci, macrolide-resistant
- Streptococcus pneumoniae, macrolide-resistant
- Haemophilus influenzae, ampicillin-resistant
- Group B streptococci, penicillin-resistant
AMR returns to the Congress agenda in Barcelona this year, so do get your tickets to be part of essential conversations on how the vaccine community can contribute to the addressing the problem, and don’t forget to subscribe for more insights here.
by Charlotte Kilpatrick | May 9, 2024 | Infection |
In May 2024, the UKHSA shared that recent data reveal cases of whooping cough “continue to increase”, with the highest burden born by infants. 1,319 cases were confirmed in March, an increase on January’s 556 cases and February’s 918 cases. This takes the total number of cases in 2024 to 2,793. Unfortunately, during this first quarter there have also been five infant deaths, with young infants being at “highest risk of severe complications and death”. While vaccine effectiveness estimates for pregnancy show “high levels of protection (92%)”, uptake is declining.
Whooping cough
Known as the “100-day cough”, whooping cough (or pertussis), is a bacterial infection that spreads “very easily”. Initial indications are like a cold, but this develops into coughing bouts, gasping for breath, or bringing up mucus. It is a cyclical disease that “peaks” every 3 to 5 years. However, due to pandemic restrictions and behaviour there was a drop in cases. A peak year is “therefore overdue”. Furthermore, the pandemic resulted in “reduced immunity in the population”.
The data in detail
From January to March 2024 there were 2,793 confirmed cases; among these cases around half (50.8%) were in people aged 15 years or older. For infants under 3 months, who are too young to be fully vaccinated, there was a peak in cases to 407 in the 2012 outbreak; this fell after the introduction of the maternal vaccine. More recently, cases in infants under 3 months increased to 48 cases in 2023. Between January and March 2024 there were 108 confirmed cases in infants under 3 months.
Uptake falls
“Vaccination in pregnancy is key to passively protecting babies before they can be directly protected by the infant vaccine programme.”
Vaccination against pertussis is recommended in “every pregnancy” between 20 and 32 weeks, “ideally after the 20-week scan”, but can be given as early as 16 weeks. After birth it is “important” for babies to be vaccinated when eligible at 8, 12, and 16 weeks.
The best defence
Dr Gayatri Amirthalingam, UKHSA Consultant Epidemiologist, reminded the public that “vaccination remains the best defence” against this disease, emphasising that it is “vital” that people get their vaccines “at the right time”.
“Pregnant women are offered a whooping cough vaccine in every pregnancy, ideally between 20 and 32 weeks. This passes protection to their baby in the womb so that they are protected from birth in the first months of their life when they are most vulnerable and before they can receive their own vaccines.”
While whooping cough can affect “people of all ages” it can be “extremely serious” for very young babies. Dr Amirthalingam offered “thoughts and condolences” to the families who have “so tragically lost their baby”.
NHS National Medical Director, Professor Sir Stephen Powis, agreed that it is “vital” that families “come forward to get the protection they need”. Professor Powis recommended that people who are pregnant and have not been vaccinated yet or have unvaccinated children “contact your GP as soon as possible”.
“If anyone in your family is diagnosed with whooping cough, it’s important they stay at home and do not go into work, school, or nursery until 48 hours after starting antibiotics, or 3 weeks after symptoms start if they have not had antibiotics.”
For more infectious disease updates make sure you subscribe to our weekly newsletters here.
by Charlotte Kilpatrick | Apr 25, 2024 | Infection |
For World Malaria Day 2024, WHO shared a message from the Director of the WHO Global Malaria Programme and emphasised the need to return to malaria progress in line with this year’s theme:
“Accelerating the fight against malaria for a more equitable world.”
WHO suggests that, in recent years, progress in reducing malaria has “ground to a standstill”, affecting health and costing lives. Furthermore, it “perpetuates a vicious cycle of inequity”. In this article we cover the message from WHO Global Malaria Programme Director, explore the key concerns shared for this year’s World Malaria Day, and share UKHSA’s update on malaria cases observed in the UK.
World Malaria Day: in pursuit of an equitable world
The theme, “accelerating the fight against malaria for a more equitable world”, highlights the fact that malaria “disproportionately” affects people who live in the “most vulnerable situations”. WHO states that the African Region “shoulders the heaviest burden” of the disease; in 2022 it accounted for 94% of malaria cases and 95% of malaria deaths. WHO reflects that the “current trajectory” indicates that we will miss critical 2025 milestones for reductions in cases and deaths.
The most likely to be affected are those who live in “situations of poverty and with less access to education”. This year, WHO is joining the RBM Partnership to End Malaria and other partners to highlight barriers to health equity, gender equality, and human rights in malaria responses worldwide, with “concrete measures to overcome them”.
Dr Ngamije’s message
Dr Daniel Ngamije, Director of the WHO Global Malaria Programme, shared a message in April 2024, highlighting the collaboration with the RBM Partnership and others. The statement begins by “acknowledging the tremendous contributions of national malaria programmes and their partners”.
“Our collective work will contribute to a more equitable future.”
However, malaria is still a “serious global health challenge” that takes the “heaviest toll on the most vulnerable”. Dr Ngamije is concerned that “too many people” are missing the services and information needed to prevent, detect, and treat malaria. This is particularly true for those “experiencing disadvantage, discrimination, and exclusion”.
“We need to strengthen and step up our support for these populations – not only is it our moral duty, it is the best way to get back on track to achieve our global malaria targets.”
Since 2017, WHO has been reporting “stalling of progress”, notably in countries that carry a high burden of disease. In 2022, malaria killed around 608,000 people and caused 249 million new cases.
“Without a change in the current trajectory, many people, especially those living in situations of greatest poverty and vulnerability, will continue to die from malaria – a disease that is preventable and treatable.”
High burden countries
Dr Ngamije identifies “health inequities” as “hampering efforts” to reduce malaria in the countries hardest hit by disease. With the “High burden to high impact” (HBHI) approach from 2018, countries have been identifying those who suffer most and responding with a “concerted effort” to provide customised packages of interventions and services.
Low burden countries
“Health inequities are also undermining efforts to complete the last mile in the pathway to eliminate malaria.”
In “many” lower burden countries, cases of malaria are “concentrated among vulnerable, hard-to-reach populations”. These populations include mobile and migrant workers, refugees, and indigenous communities.
“Reaching, engaging, and empowering these populations with targeted, gender-responsive, and culturally sensitive interventions and services is an important strategy for achieving our collective vision of a malaria-free world.”
Yaoundé Declaration
In March 2024, Ministers of Health from HBHI countries demonstrated “further political commitment” as they signed the Yaoundé Declaration in Cameroon. This declaration signified Ministers’ commitment to providing “stronger leadership and increased domestic funding for malaria control programmes”, ensuring investment in data technology, applying the latest technical guidance, and enhancing control efforts at all levels.
The declaration demands that countries “sustainably and equitably” address the challenge of malaria, with Ministers recognising the importance of “tackling the root causes of stagnating progress in malaria control”. Further commitments relate to ensuring all populations at risk of malaria “consistently receive the appropriate tools”.
What are WHO and partners doing?
The global malaria response can be strengthened by increased investment into the research and development of new tools to benefit anyone who is at risk, especially the “poorest and most marginalised populations”. WHO hopes that recommended tools will be scaled up in an “equitable and sustainable way”. For example, recent recommendations, such as dual active ingredient nets and malaria vaccines, could increase health equity for populations at risk of malaria.
WHO also suggests that the fight against malaria can be accelerated through a commitment to UHC (universal health coverage).
“Everyone should have access to the health services they need – when and where they need them, and without facing financial hardship.”
WHO recommends reorienting health systems towards primary care, which is understood to be the “most inclusive, equitable, and cost-effective way to achieve UHC”. A recent operational strategy from the Global Malaria Programme has the “potential to shape the malaria ecosystem and achieve impact at country level”. The strategy emphasises that efforts to fight malaria should be “rooted in the principles of health equity, gender equality, and human rights”.
UKHSA data
In advance of World Malaria Day, UKHSA shared data that reveal an increase in malaria cases across England, Wales, and Northern Ireland. Reported cases exceeded 2,000 for the first time since 2001, with cases confirmed in individuals who had “recently been abroad”. The number of cases is described as a sign of the importance of “taking precautions” while travelling abroad.
In 2023 there were 2,004 cases of malaria confirmed after international travel, which compares with 1,369 in 2022. UKHSA links this rise to a “resurgence of malaria in many countries” and an increase in overseas travel as pandemic restrictions were lifted.
ABCD and commentary
UKHSA shares the ABCD of malaria prevention: “Awareness of risk, Bite prevention, Chemoprophylaxis, and Diagnose promptly and treat without delay”. This method can ensure that travellers are protected as they follow travel advice for their destination. There are currently no licensed malaria vaccines for travellers.
Professor Peter Chiodini is Director of the UKHSA Malaria Reference Laboratory (MRL) and remarked that “all malaria cases are preventable”, with “simple steps” reducing infection risks.
“While malaria can affect anyone, the majority of Plasmodium falciparum malaria cases in the UK occur in those of African background. Even if you have visited or lived in a country before, you will not have the same protection against infections as local people and are still at risk.”
Professor Chiodini is working “in partnership with communities at greater risk” to improve access to and use of “effective” malaria prevention measures. Dr Dipti Patel, Director of the National Travel Health Network and Centre, encouraged travellers to “prioritise” their health and “plan ahead”.
“Check the relevant country information pages on our website, TravelHealthPro, and ideally speak to your GP or travel health clinic 4 to 6 weeks ahead of travelling to ensure you have had all the necessary vaccinations and advice you need to ensure your trip is a happy and healthy one.”
At The World Vaccine Congress malaria continues to be a topic of priority and we look forward to continuing these conversations with the community. Do make sure you have subscribed to our weekly newsletters here for more information and insights.
by Charlotte Kilpatrick | Mar 27, 2024 | Global Health |
A survey from the UKHSA, shared in March 2024, reveals that “most” parents in England have a “positive view” of the childhood immunisation programme and consider healthcare professionals the most trusted source of information. The 2023 annual parental attitudinal survey shows that 89% of parents agree that vaccines work, with 84% agreeing that they are safe and 82% agreeing that they are trusted. The online survey was open to parents of children between the ages of 2 months and 5 years and was conducted by the commercial research organisation BASIS.
Survey findings
Around 1,000 respondents had a child aged between 2 months and 3 years, 4 months, and 1,000 respondents had a child aged 3 years, 4 months to less than 5 years. The most frequently recalled health issue that parents had seen or heard about in the past 12 months was respiratory syncytial virus (RSV), followed by ‘healthy eating’ (37%). Vaccines, apart from the COVID-19 vaccines, were “spontaneously” recalled by 34% of parents. However, when prompted, 73% of parents reported having seen or heard something about vaccines (including COVID-19 vaccines) for children in the previous 12 months.
Serious diseases
The diseases that parents were most concerned about were rated “very serious”; these were septicaemia (86%) and meningitis (81%). RSV was rated as “very serious” by 58% of parents to babies and younger children, which was higher than in parents of slightly older children. Flu was perceived as less serious, with only 19% of all parents rating it as “very serious”.
Vaccine safety and confidence
A total of 88% of parents were happy with the safety of vaccines offered to babies and young children. However, this is a reduction from the 2022 survey, which found 92% happy.
“Parents in social grade C2DE and ethnic minorities were more likely to report feeling less happy with the safety of vaccines for babies and young children.”
The survey found that 89% of parents agreed that vaccines work, that they are safe (84%), and trusted (82%). Although UKHSA recognises that these are “high”, the levels are again lower than the 2022 survey.
Information sources
77% of parents reported seeing or hearing information about vaccines for babies and young children from “approved” sources such as healthcare professionals, the NHS website or leaflets, or the child’s personal health record (known as the Red Book). Of the 67% of parents who reported seeing vaccine information online, almost a third of them had seen it on the NHS website and 18% on parenting websites like Mumsnet.
Facebook was the most commonly reported social media source (24% of parents who had seen information online). Instagram, Twitter, and Snapchat were also cited as sources. Women were “more likely than men” to see or hear about vaccines through healthcare professionals and men were “more likely” to have heard about vaccines for their child through social media/online, or through friends and family.
72% of parents who had seen or heard something about vaccines in the last 12 months reported that the information had been in favour of vaccines. Again, this was lower than the 2022 survey (80%). 59% of parents had not seen or heard anything that would cause concern about any childhood vaccines.
When respondents were asked to rank different sources of information:
- 86% ranked the NHS in 1st-3rd place
- 85% ranked health professionals (like a GP, practice nurse, midwife, or health visitor) in 1st-3rd place
- 66% ranked pharmacists in 1st-3rd place
- Only 10% ranked the internet in 1st-3rd place
- Only 5% ranked social media in 1st-3rd place
Vaccine conversations
86% of all parents felt they had received enough information to make an “informed decision” about the vaccines offered to their children. This was higher than the 81% of parents who reported this in the 2022 survey. 86% of parents of younger children reported that they had an opportunity to discuss childhood vaccination with a health professional before their child’s first vaccines; 18% reported a discussion before the baby was born; 46% had the discussion soon after birth, and the rest had the discussion at the vaccination visit (22%).
Health visitors (56%) and midwives (43%) were the health professionals most commonly reported as having vaccine discussions with parents. 83% of parents had already decided that their babies would have all the vaccines offered before they had a discussion. 14% who had not made up their minds decided in favour of vaccination after the discussion.
“Ethnic minorities, men, and younger parents were more likely to have changed their mind and decided to have their baby vaccinated after speaking to a healthcare professional.”
Around 80% of parents were either satisfied or very satisfied with their most recent vaccine experiences.
Parents have confidence
Dr Mary Ramsay, Head of Immunisation at UKHSA, commented on the results.
“The recent survey shows that most parents have confidence and trust in the NHS childhood vaccination programme and it’s reassuring to see that 86% of parents say that NHS resources and healthcare professionals are their most trusted sources for information.”
While Dr Ramsay emphasised that “it’s completely natural” for parents to have questions, the survey highlights “just how important healthcare professionals are in ensuring parents get to know the facts”. She urged parents to “speak to their GP, midwife, health visitor, or other trusted healthcare worker or visit nhs.uk for the latest advice and answers to common questions.”
“All parents want to do the best for their children – ensuring your child receives all their vaccines on time is one of the most important things you can do to help give them the very best start in life.”
Steve Russell, NHS Director of Vaccinations and Screening, stated that “vaccination is one of the most important tools to save lives and prevent disease”, so it’s “great” to see that the NHS is the “source most people trust”.
“It is never too late to have this conversation to help you and your family make an informed choice. Anybody who wants to discuss what vaccinations they are eligible for should contact their GP practice.”
For more on the importance of trust in ensuring uptake of routine immunisation programmes, join us at the Congress in Washington this April or subscribe to our newsletters here.
by Charlotte Kilpatrick | Mar 13, 2024 | Infection |
In March 2024 the UK Health Security Agency (UKHSA) announced that a new collaboration with The Pirbright Institute has been launched to support the development of vaccines against henipavirus, the genus that includes Nipah virus, with funding from the Medical Research Council. UKHSA scientists will use a model of Nipah virus disease to evaluate vaccines developed by the Pirbright Institute to determine protective effects.
Nipah virus
With a high case fatality rate and no licensed vaccines or treatment, Nipah virus is a “current and future threat” to global health. It is currently on WHO’s priority pathogen list and has caused recent outbreaks in Bangladesh and India. While there have not been recorded cases in the UK, the UKHSA recognises that effective vaccines could provide protection to people in countries where the virus is endemic, with the secondary effect of preventing imported cases.
Nipah virus is part of the henipavirus genus, and UKHSA states that there is a possibility for the emergence of a novel virus with outbreak potential. Thus, instead of focusing on a specific virus target for vaccination, the aim is to develop a vaccine that provides “cross protection against the whole genus” (pan-henipavirus vaccine).
Professor Isabel Oliver, Chief Scientific Officer at UKHSA, hopes that the study will “deepen our understanding of henipaviruses” and encourage “significant progress in our efforts to protect health from this current and future global health threat”.
“The work will also make a vital contribution to the 100 Days Mission – an important initiative to make sure the world is better prepared for the next pandemic by accelerating the development of diagnostics, therapeutics, and vaccines.”
Dr Dalan Bailey, Viral Glycoproteins group leader and project lead for Pirbright, emphasised that the project represents a “really important first step in the development of broadly acting vaccines”.
“This is especially important as we try to build more robust pandemic preparedness plans in the wake of the COVID-19 pandemic, and we are delighted to be working with UKHSA on this project.”
Professor Oliver will join us at the Congress in April to discuss approaches to some of the most challenging and threatening pathogens so do get your tickets to hear more from her or subscribe to our newsletters here.
by Charlotte Kilpatrick | Mar 8, 2024 | Infection |
In March 2024 the UKHSA revealed that new data show a “continued increase” in cases of pertussis (whooping cough) at the start of the year. The statement from the agency indicates that this increase comes after a “prolonged period of low case numbers” due to COVID-19 restrictions. Although cases of whooping cough “rise cyclically every few years”, UKHSA is concerned that there has been a “steady decline in uptake” of the vaccine in pregnant women and children. Whooping cough is a bacterial infection that affects the lungs.
January data
The data show a dramatic increase compared to the whole of the previous year (2023). In January, there were 553 confirmed cases in England, whereas the country reported a total of 858 in 2023. In 2016 there was a peak in cases with 5,949. The data also reveal that 22 infants under the age of 3 months were diagnosed with whooping cough. These children, too young to be fully vaccinated, are at “greater risk of severe disease” and death.
With the increase taking off so quickly already, the UKHSA has moved to a monthly reporting cycle for whooping cough infections to offer “timely information” on disease rates. This will allow public health teams to respond to outbreaks and support health professionals as they deliver the routine vaccination programme.
Get protected
In response to the increase in cases, UKHSA is encouraging pregnant women to get protected so that their newborns are protected. It states that vaccination of pregnant women is 97% effective at preventing death in infants from whooping cough. Furthermore, parents and carers are urged to check that their children are vaccinated. The current schedule offers vaccines to infants at 8, 12, and 16 weeks old (within the 6-in-1 combination vaccine), with a further dose in the pre-school booster vaccine.
Unfortunately, a recent decline in uptake of vaccinations has become noticeable; the number of 2-year-olds who had completed their 6-in-1 vaccinations by September 2023 was at 92.9%, which was lower than 96.3% in March 2014. Furthermore, uptake of the maternal pertussis vaccine, which is offered to every woman in pregnancy, dropped from over 70% in September 2017 to around 58% in September 2023.
The new campaign
The latest reminders feature in the UKHSA’s recent Childhood Immunisation Campaign, which calls upon parents and carers to check that their children are protected against measles and other serious diseases. Dr Gayatri Amirthalingam, Consultant Epidemiologist at UKHSA, commented that, while whooping cough “can affect people of all ages”, it can be “particularly serious” for very young infants.
“However, vaccinating pregnant women is highly effective in protecting babies from birth until they can receive their own vaccines. Parents can also help protect their children by ensuring they receive their vaccines at the right time or catching up as soon as possible if they have missed any.”
Steve Russell, National Director for Vaccinations and Screening at NHS England, emphasised the importance of families taking the protection offered by the vaccine.
“If you are pregnant and have not been vaccinated yet, or your child is not up-to-date with whooping cough or other routine vaccinations, please contact your GP as soon as possible, and if you or your child have symptoms ask for an urgent GP appointment or get help from NHS 111.
For more on encouraging vaccine uptake and protecting vulnerable populations, join us in Washington for the Congress this April, or subscribe for insights here.
by Charlotte Kilpatrick | Mar 7, 2024 | Technology |
In March 2024 the UK Government announced that AstraZeneca plans to invest £650 million in the UK to boost the “world leading Life Sciences sector” and “grow the economy”. The investment is expected to “enhance public health protection and pandemic preparedness”.
Vaccine investments
AstraZeneca reportedly intends to invest £450 million at the manufacturing site in Speke, Liverpool, to support the research, development, and manufacture of vaccines. The site already provides a “world leading childhood vaccination programme”. The new facility will be designed and built to be “operationally net zero” with power from renewable energy sources.
Further support for the UK’s “resilience for future pandemics and global health threats” comes in the plan for an AstraZeneca partnership with UKHSA to advance science for developing and evaluating vaccines with technology from the site in Speke and the UKHSA’s Vaccine Development Evaluation Centre (VDEC) at the site in Porton Down. Also planned is the expansion of AstraZeneca’s presence at “Europe’s largest life sciences cluster” in Cambridge, with a £200 million investment. The facility is set to house around 1,000 employees, providing opportunities and benefits such as National Insurance cuts.
The UK’s economic plan
In the statement, the UK Government describes its tax regime as “one of the most competitive” of any major economy: “sticking to an economic plan to build a stronger economy where hard work is rewarded, and ambition and aspiration are celebrated”. AstraZeneca’s plans are the “latest step” in a plan to “deliver the long-term change that Britain needs”.
The Chancellor, Jeremy Hunt, commented that “we’ve delivered one of the most competitive business tax regimes of any major economy” within the plan to “help our key industries to grow”.
“Our £108 billion Life Sciences sector provides over 300,000 high skilled jobs across the UK and is crucial for the country’s health, wealth, and resilience.”
Mr Hunt is “sticking to our plan” to make the UK “one of the best places” to invest in the development and manufacturing of “new, innovative medicines”. AstraZeneca’s Chief Executive Officer, Sir Pascal Soriot, believes the planned investment will “enhance the UK’s pandemic preparedness” and is a sign of “ongoing confidence in UK life sciences”.
“We will continue to support the UK in driving innovation and patient access, building on the strong foundations which have been put in place.”
Sir Soriot is “proud” of AstraZeneca’s “British roots” and how far the company has come since the merger of UK and Swedish Zeneca Group and Astra AB.
“We are now a truly global company that has transformed the lives of millions of patients throughout the world with a relentless focus on science and innovation.”
Chief Scientific Officer at UKHSA, Dr Isabel Oliver, stated that the investment will “bolster the development of the UK’s vaccine capabilities and life sciences sector”. These are “critical components of the country’s resilience to future health threats”.
“UKHSA majors on researching and developing new ways to strengthen the country’s defences against all health hazards – including future pandemics – and works routinely with a range of commercial and academic partners.”
Victoria Atkins is the Health and Social Care Secretary, who described the UK as a “global leader in the research and development of life saving vaccines”.
“Today’s announcement is testament to this country’s Life Science capabilities – and our continued commitment to pandemic preparedness and global health. As well as creating new highly skilled jobs, this investment will help maintain the UK’s position at the forefront of tackling emerging diseases and support our work to make our healthcare system faster, simpler, and fairer.”
To hear more from senior representatives of both AstraZeneca and UKHSA at the Congress in Washington this April, get your tickets here and don’t forget to subscribe for more vaccine investment insights.
by Charlotte Kilpatrick | Feb 29, 2024 | Global Health |
In February 2024 UKHSA announced that a new marketing campaign is to be launched across England to “remind parents and carers” of the risks their children face from “serious diseases that are re-emerging in the country”. The “urgent call to action” is to catch up on missed vaccinations. The campaign will go live on 4th March with a video advert from the perspective of children.
“If we’re not vaccinated, we’re not protected.”
Responding to a need
The theme and materials were reportedly developed in response to consultations with parents in the North West. The campaign comes amid rising numbers of measles cases across the country; the latest weekly update reported a total of 69 cases, bringing the total number of laboratory confirmed measles cases to 650 since 1st October 2023.
UKHSA Chief Executive Professor Dame Jenny Harries will visit sites in Manchester and Liverpool to launch the campaign; parts of the North West have “some of the lowest uptake rates” in the country. Areas with low uptake will be in focus for support and parents of children between the ages of six and eleven will be contacted and encouraged to make an appointment for missed MMR vaccines.
The campaign features a television advert, radio advertising, and social media efforts. Further advertising will be shown in the West Midlands, North West, and London, where there are “larger pockets of low uptake”.
Falling uptake
UKHSA states that uptake levels of childhood vaccines that are available through the NHS routine vaccination programme in England have been “falling over the past decade” across “all vaccines, from whooping cough to measles, mumps, and rubella, and polio. England no longer has the necessary levels of population immunity recommended by WHO to prevent outbreaks.
Professor Dame Jenny Harries commented on the need for an “urgent reversal of the decline” in vaccine uptake to “protect our communities”
“Through this campaign we are particularly appealing to parents to check their children’s vaccination status and book appointments if their children have missed any immunisations. The ongoing measles outbreak we are seeing is a reminder of the very present threat.”
Although much of the country is protected, Professor Dame Harries is concerned about “high numbers of children in some areas” that are “unprotected from preventable diseases”. Indeed, the risk is not only to “their own health”, but that of “other unvaccinated people around them”.
“Unless uptake improves, we will start to see the diseases that these vaccines protect against re-emerging and causing more serious illness.”
The best for children
Maria Caulfield, Health Minister, recognises that “parents want what is best for their children”, and stated that this “includes the vital protection that vaccines provide from preventable diseases”. The campaign will be an “important step to engage local communities and highlight the importance of immunisation”, particularly as “diseases like measles are not illnesses of the past”.
“We want to make sure parents know how and where they can get essential jabs for their children as quickly as possible. I want to encourage parents to get their children immunised, particularly if they are behind on their immunisation schedule.”
Steve Russell is National Director for Vaccinations and Screening at NHS England and emphasised that the MMR vaccination “offers the best protection against becoming seriously unwell”. Although the increase in measles cases “is a global issue”, NHS England is “doing all it can” to support communities and offer the “best possible protection”. This involves sending reminders to parents and guardians of children under five and asking all parents and guardians of children between six and eleven to ensure their children have the “maximum protection” of two doses.
“Measles is a serious illness, and in some cases can lead to having to be admitted to hospital for treatment, so the message is clear: if you or your young ones aren’t vaccinated, you aren’t protected, and it is vital you come forward as soon as possible.”
Dr Linda Charles-Ozuzu, Regional Director of Commissioning for NHS England North West, highlighted that “routine vaccinations have been given to generations of children” and “proven to be effective at preventing serious childhood illnesses”. Not only do these vaccines protect the vaccinated but “those who are too young to be vaccinated” and “people who are vulnerable” who benefit from “herd immunity”.
“With the health of some children at risk because of falling vaccination rates, we really hope this campaign will help to remind parents about the important role childhood vaccines play and encourage them to bring their children forward when they are invited.”
To participate in discussions about vaccines for emerging and re-emerging diseases and to hear more from senior representatives of UKHSA, do join us at the Congress in Washington this April by getting your tickets here. If you can’t make it, why not subscribe for more updates?
by Charlotte Kilpatrick | Jan 25, 2024 | Technology |
In January 2024 the UKHSA published its Pathogen Genomics Strategy, which sets out a 5-year plan for the organisation’s role in the “wider delivery of pathogen genomics to prepare for and respond to infectious disease threats to public health”. Acknowledging the important of pathogen genomics on public health, particularly in the pandemic response to SARS-CoV-2, the UKHSA hopes to “integrate genomics into aspect of infectious disease control”. Priority will be given to areas of “vaccine-preventable disease, emerging infections, and antimicrobial resistance”, in which pathogen genomics has the “potential to yield substantial measurable benefits in health security”.
The strategy at a glance
The Strategy outlines the “direction” of investment in pathogen genomics to “mitigate public health threats from infectious diseases” and support delivery of the Science Strategy and organisational strategic plan.
“Over the next decade we aim to maximise the benefit of pathogen genomics for public health and health security, through a single co-ordinated programme across the agency working with the NHS, academic partners, industry, other Government Departments, and devolved administrations.”
The programme will “improve” understanding of pathogens that post the greatest risks to the UK population, “integrate genomics into every day public health decision making”, and “enhance the evidence base” for policy.
“We will improve health security, detecting and containing outbreaks, improving and protecting our vaccines and therapeutics, and building our capabilities to detect new pathogens and threats.”
Through seven strategic, “cross-cutting aims”, and three priority public health areas, the UKHSA outlines a “vision” for the next five years.
Strategic aim 1: use genomic data to optimise clinical and public health decision-making, from local to global settings
The following objectives are presented:
- Integrate pathogen genomic data into public health systems: we will ensure that pathogen genomic data is linked to epidemiological data and incorporated into clinical and public health systems to improve disease control and to quickly identify and respond to public health threats.
- Develop best practice guidelines for pathogen genomic data use: we will work with partners to develop consensus on genomic data standards and develop guidelines for how, when, and where pathogen genomic data should be used to inform clinical and public health decisions for all communities.
- Evaluate and implement metagenomic analysis: we will work with NHS England to investigate the utility of metagenomic analysis to quickly and accurately identify pathogens causing disease, including pathogens present in the environment, and design novel surveillance systems to enhance biosecurity.
Strategic aim 2: use genomic data to drive improvements in diagnostics, vaccines, and therapeutics.
The following objectives are presented:
- Use pathogen genomic data to inform vaccine development: we will use genomic data to help ensure that existing vaccines continue to be effective against current and emerging strains of pathogens, whilst using genomic data to inform development of new vaccines.
- Enhance therapeutic development and deployment using pathogen genomic data: we will use pathogen genomic data to understand the extent and evolution of antimicrobial resistance, enabling more effective treatments to be targeted to patients and informing future drug development.
Strategic aim 3: Provide a nationally coordinated, high-throughput pathogen genomics sequencing and analysis service
The following objectives are presented:
- Ensure that infrastructure and partnerships are in place to sequence and analyse large volumes of pathogen genomic data at pace to inform clinical decision-making: we will work to deliver scalable, robust, and standardised laboratory services, bioinformatic analysis pipelines and translational services for priority pathogens.
- Foster pathogen genomics system resilience and adaptability: working across UKHSA, we will build a system which is resilient, scalable, and rapidly adaptable to new public health challenges.
- Ensure equitable access nationally: working with stakeholders, including partners in the devolved nations, ensuring consistent, effective access to and use of pathogen genomics laboratory techniques, data, analysis, and infrastructure across the UK.
Strategic aim 4: Undertake a genomics workforce transformation within and beyond UKHSA
The following objectives are presented:
- Strengthen clinical and scientific genomics expertise and training: we will ensure there are clear pathways for the development of specialists in all aspects of pathogen genomics, from sequencing to policy applications.
- Improve genomic literacy across clinical and public health: working with stakeholders, we will develop training packages to improve the understanding and use of genomic data across all levels of the clinical, scientific, public health, and policymaker workforce.
Strategic aim 5: Commit to pathogen genomic data sharing and global collaboration
The following objectives are presented:
- Enable rapid public data sharing: we will support the development of national and global policies, systems, and infrastructure to ensure that pathogen genomic data is quickly and fully shared with the global public health community and researchers.
- Foster collaborative networks: building on existing networks and working with key multilateral agencies, we will foster partnerships between organisations and countries to enhance the sharing of genomic data and scientific knowledge and improve global health security and response capabilities.
Strategic aim 6: Drive innovation in pathogen genomics
The following objectives are presented:
- Set priorities for health protection and security research and development in pathogen genomics: we will work across government, develop priorities with academic funders, work with academic partners thrgouh NIHR HPRU, joint grants and academic partnerships, and promote collaboration and knowledge exchange with a focus on improving the evidence base for linking human and pathogen genomics, developing methodologies and cost-effectiveness estimates.
- Develop innovation hubs: we will work to connect academic, NHS England Centres of Excellence, and industry partners to find pragmatic solutions for priority public health challenges.
- Develop industry partnerships: we will work with companies who develop sequencing technologies, bioinformatic tools, diagnostic platforms to leverage resources and support the UK ambition to enhance productivity across the economy, and in turn bring jobs, growth, and prosperity to all parts of the UK.
Strategic aim 7: Build high-impact services that are good value for money
The following objectives are presented:
- Develop and conduct rigorous health economic evaluation: we will embed evaluation of public health impact and value for money into our services, and build the evidence base for the value of pathogen genomics for public health.
- Ensure long-term sustainability: through improvements in laboratory efficiency, we will work to ensure that our genomic services are sustainable and continue to deliver value over the long-term. We will also improve flexibility to keep pace with advances in technology and the expanding role of pathogen genomics.
Three key areas
The strategic aims “cut across” three areas that are “directly aligned” with UKHSA’s strategic priorities, chosen for their population health impact and because “investment in pathogen genomics and its application in these areas offers evidence-based public health benefits”.
- AMR: Pathogen genomics applied to AMR will provide detailed understanding of resistance mechanisms and transmission patterns, enabling healthcare practitioners and policymakers to implement targeted infection control interventions and antimicrobial stewardship programmes, ultimately preserving the efficacy of antibiotics and protecting public health.
- Emerging infections and biosecurity: Pathogen genomics will serve as an early-warning system for emerging infections, facilitating the detection and rapid and precise identification of new or variant pathogens. This capability will guide timely public health responses and strengthen biosecurity, and mitigate the impact of public health threats.
- Vaccine-preventable diseases and elimination programmes: The application of pathogen genomics to vaccine-preventable diseases will inform vaccine development and deployment, support the identification and interruption of disease transmission chains, and play a role in achieving disease elimination targets, ultimately contributing to improved vaccine efficacy and enhanced population immunity.
The experts weigh in
Dr Meera Chand, Deputy Director for Emerging Infections and Clinical Lead for the Genomics Programme at UKHSA, commented that pathogen genomics is an “essential component of world’s ability to respond quickly to infectious disease threats”.
“The new UKHSA Pathogen Genomics Strategy will provide a framework for us to build on our already substantial capacity in this area, and to implement genomics across all our work to keep the public safe from threats to their health.”
UKHSA Chief Executive, Professor Dame Jenny Harries, emphasised the “vital contribution” pathogen genomics experts in the COVID-19 pandemic response.
“Pathogen genomics remains central to the national and international effort to keep the public safe from many other types of infectious disease threats.”
It will be “even more important” for the future, suggested Professor Harries, who hopes that the new strategy will “ensure that UKHSA continues to be at the forefront of implementing this technology to keep our communities safe, save lives, and protect livelihoods.”
We look forward to welcoming senior representatives of the UKHSA to our Congress in Washington once again; will you join us to learn more? To check out their sessions on the agenda, click here. Don’t forget to subscribe for weekly updates like this.
by Charlotte Kilpatrick | Jan 19, 2024 | Infection |
In January 2024, as a “rapid rise in cases” is observed in the UK and other countries, the UKHSA Chief Executive has called for “immediate action” to increase measles, mumps, and rubella (MMR) vaccination uptake. This trend in cases has been observed since October 2023, with at least 216 confirmed cases and 103 probable cases in the West Midlands. UKHSA reports that around 80% of these cases have been identified in Birmingham, and most patients are children under 10 years old. The UKHSA has declared a “national incident”, which signals the “growing public health risk” and allows the Agency to focus on limiting the spread.
Measles is highly infectious among the unvaccinated, especially in nurseries and schools. It can be “very unpleasant” and can be “very serious” for some children, leading to hospitalisations or deaths in rare cases. Furthermore, people in some high-risk groups are at increased risk of complications. Luckily, there is a safe and effective vaccine; over 99% of people who have had both doses are protected against measles and rubella. It also protects against mumps, in a slightly lower capacity.
Professor Dame Harries visits Birmingham
On 19th January, Chief Executive Professor Dame Jenny Harries visited Birmingham to engage with the “extensive clinical, health protection, epidemiological, and community engagement work” that is being carried out to contain the spread. Dame Harries has expressed “concern” that, due to some areas having low MMR vaccine uptake, there is a risk of the virus spreading.
In Birmingham, Dame Harries will visit the Birmingham Heartlands Hospital and meet with health professionals who are coordinating the response across the West Midlands. The UKHSA states that “learning what has worked and not worked” in this outbreak will be “key” to empowering other areas. Given examples include “successful interventions” like a pop-up vaccination clinic at a school in Coventry, street level community engagement on the importance of vaccination, and training and awareness raising of frontline professionals.
A need for action
Dame Harries recognised the work of her colleagues in “tirelessly” trying to control the outbreak but warned that “with vaccine uptake in some communities so low, there is now a very real risk of seeing the virus spread”.
“Children who get measles can be very poorly and some will suffer life changing complications.”
Dame Harries recommends parents protect their children by ensuring they get the MMR vaccine, with two doses offering “lifelong protection”. She emphasised that it is “never too late to catch up”.
“Immediate action is needed to boost MMR uptake across communities where vaccine uptake is low. We know from the pandemic that the communities themselves, and those providing services within them, will have the knowledge to best support local families to understand the risks of measles, to learn more about the vaccines that can protect them, and to enable innovative vaccine delivery approaches.”
She called for a “long-term concerted effort” to encourage protection and prevent “large” measles outbreaks.
Vaccination Strategy
The NHS England Vaccination Strategy was welcomed by UKSA in December, and it emphasised a focus on innovative delivery approaches. The UKHSA is committed to supporting national vaccination programmes, particularly MMR, which is part of the NHS Routine Childhood Programme. Doses are offered at 1 year old and again at 3 years 4 months. The vaccine is free, and parents are urged to check if their children have had both doses.
For more on routine immunisation efforts and increasing vaccine uptake, join us at the Congress in April in Washington. Until then, why not subscribe for regular immunisation updates?