An article for BMJ Global Health in January 2024 states the importance of moving in the direction of “global vaccine equity with shared goals, intermediate steps, and long-term advocacy goals”, with an emphasis on doing so “before the next pandemic”. Recognising that “vaccines are key to preventing and ending pandemics”, the authors state that COVID-19 “will not be the last pandemic” and invite countries to use lessons from their experience of it, as well as their responses to the HIV pandemics. They describe the HIV response as “at the vanguard of ensuring equitable access to rights-based services, to create shared goals and engage communities to increase access to and delivery of safe, quality vaccines”.
COVID-19 and inequality
Even though COVID-19 is known to have been a “leading cause” of morbidity and mortality globally, resulting in “almost 7 million deaths” by January 2023, many cases were undetected due to “widespread lack of diagnostic test availability”. Therefore, the human burden is underestimated. Although vaccines have “been essential” in reducing this burden, countries “scrambled” to access them, which meant that “the most effective vaccines largely went to countries in the Global North” at the start.
For example, the Africa region represents one-fifth of the global population but had only received 3% of all COVID-19 doses by 2021.
“While the number and types of vaccines delivered to the Global South have increased over time, countries in the Global South have been the most disadvantaged in obtaining access to the most effective vaccines.”
Vaccine equity
The authors consider “two central dimensions” for vaccine equity:
Access – are the vaccines a country has the most effective vaccines available? Are the prices for the vaccines affordable for the country?
Delivery – Does the country have a quality healthcare system, supply chain, and workforce to deliver the vaccines?
Even within countries, vaccines have been distributed “unequally”, usually to the disadvantage of the most vulnerable, including “people with disabilities, homeless populations, refugees, as well as those in prisons, crowded living conditions, and with precarious work conditions”. Furthermore, those living with HIV who are not virally suppressed are at “high risk” of COVID mortality. The article highlights that of the 38 million people who live with HIV, more than 25 million live in Africa, which has the lowest rates of COVID vaccination.
“While public health dictates that those at highest risk should be the highest priority to be vaccinated, one reason this did not occur is that individuals who had resources or were in positions of power were vaccinated first.”
This persists, despite recognition that, to limit mutations and further spread, we need to vaccinate a global majority. Therefore, the authors distil policy-level recommendations and actions for consideration by Global South country leaders.
“Given how little progress has been made to date, in an effort to ‘decolonise’ global health, countries in the Global South and CSOs may want to consider what actions to take now that will not solely depend on the goodwill of the Global North.”
Increasing access
Decentralise the production of vaccines, fostering the increased production of mRNA vaccines on many continents rather than relying on donations. The authors call for the development of a “transparent, web-based system” to monitor the supply chain that supports vaccine developers and manufacturers. They highlight that donations from the Global North are a “short-term, not perfect solution” that perpetuates dependency on donors.
Create a system of price transparency for vaccines. For example, COVAX is a public-private partnership founded to deliver COVID vaccines globally, but it did “not meaningfully” engage countries in the Global South or CSOs.
“Transparency of pricing could be a way to obtain the lowest price for low-income countries in the Global South, following the model established by UNICEF for childhood vaccines.”
Collect easily understandable, accessible, and transparent data on COVID vaccines. The authors suggest a website with the following information:
What is the effectiveness of different vaccines against which variant to prevent mortality?
Where are the different vaccines available?
Where is a particular vaccine useful given a country’s infrastructure?
Safety profile of the different vaccines
Cost per dose of vaccine in each country
Create demand for a new international legal framework that allows intellectual property (IP) rights to be waived quickly once a global pandemic is identified. Although the most effective vaccines with the fewest side effects were the mRNA vaccines developed by Pfizer and Moderna, US law “encourages grantees to protect their findings as IP”, to be sold to pharmaceutical companies which are unlikely to undertake development without profit guarantee.
“An ongoing global advocacy strategy by Global South governments, CSOs, and multilateral and bilateral organisations pressuring the Global North to engage in improved global vaccine equity is needed.”
A model for this could be based on HIV-focused efforts, as the authors highlight that the AIDS pandemic showed that “public advocacy leads to results”.
“We recommend that countries work simultaneously to both build their own mRNA vaccine production, supply, and expertise, as well as negotiating with pharmaceutical companies.”
Draw on the expertise of scientists in pharmaceutical companies around the world and other expert scientists globally who are willing to share and collaborate. Although mRNA vaccines are “new technology”, and access to this kind of expertise is “challenging”, the authors refer to Afrigen scientists receiving training and a US-South Africa-Thailand partnership to conduct manufacturing in line with GMP and share other scientific information.
Improving delivery
Create or strengthen public health systems that can deliver vaccines and other healthcare services throughout the lifespan that will lead to a reduction in morbidity and mortality.
“There is an ongoing need to create an adequate cadre of health workers, with sufficient remuneration and with the resources needed to succeed.”
Furthermore, specific laws might be required to protect healthcare workers and ensure fair working conditions. Donors can get involved by investing in “creating community demand and decision-making”. A “practical goal” for pandemic preparedness is the 7-1-7 target for detection, notification, and response: this allows primary care 7 days to assess a suspected outbreak, 1 day to notify public health authorities, and 7 days to implement effective responses.
Vaccinate strategically, vaccinating as many as possible, particularly those at highest risk, with available vaccines to reduce mortality. The authors highlight Vietnam’s use of non-pharmaceutical interventions in advance of vaccination campaigns and “massive diffusion of all media” until the country had access to vaccines.
Based on public health criteria, create an equitable system of prioritisation for gaining access to vaccines. The healthcare workers and providers must be “among the first to gain access” to lifesaving vaccines in a “functional” health system.
We recommend to either create and/or strengthen national regulatory agencies (NRAs) to appropriately regulate vaccines, ensuring that any manufacturing of vaccines meets GMP standards. Countries need transparent and effective NRAs, and where they do not have their own, they can “draw on regional regulatory systems” such as the Caribbean Regulatory System.
Identify credible, trusted sources of health information, promote health literacy and create a national scientific advisory committee to disseminate accurate and reliable information during a pandemic. Improved health literacy encourages an understanding of changing guidance in response to emerging data. All platforms that can be “interactive, trusted, and transparent” should be used and balanced with the “needs and concerns of the population”.
Foster transparent surveillance systems. Improving birth and death registrations and sharing these data can inform accurate pandemic information.
Conclusions
“A number of the interventions suggested as a way forward to move towards global vaccine equity may take varying lengths of time to institute, so therefore, it is critical to start now to take action for the future.”
The authors state that from a “moral ethical” position and the view of “reducing preventable mortality globally”, it is important that vaccine equity is a goal with “practical intermediate steps and long-term advocacy goals”.
“Scientific integrity, transparency, accountability, and clear communication will be key.”
How do you think these recommendations could be effectively implemented both in the immediate future and as we try to make pandemic preparedness a more established approach? Many of the issues that are explored throughout the paper will be considered at our Congress in Washington this April; are you joining us there? Until then, don’t forget to subscribe for more global health insights!
In January 2024 Combating Antibiotic-Resistant Bacteria Biopharmaceutical Accelerator (CARB-X) announced that it is awarding US$633k to Intravacc for the development of a vaccine that prevents Neisseria gonorrhoeae infections. Neisseria gonorrhoeae causes gonorrhoea, the second-most reported bacterial STI.
WHO reports that in 2020 there were an estimated 82 million adult infections. When left untreated, gonorrhoea can cause severe complications such as ectopic pregnancy or infertility and can lead to an increased risk of contracting HIV. People with gonorrhoea do not always notice symptoms, which means that reported cases only scratch the surface. In newborns, untreated gonococcal conjunctivitis can lead to blindness.
Developing a powerful tool
Dr Erin Duffy, R&D Chief at CARB-X, reflected that “drug-resistant strains of Neisseria gonorrhoeae have evaded all but one existing antibiotic”.
“Vaccines are powerful tools in the prevention of bacterial infections. With an appropriate vaccination strategy, Intravacc’s vaccine project, if successful, could prevent the disease, and significantly curb the spread of resistant bacteria across the globe.”
OMV vaccine
Intravacc’s meningococcal outer membrane vesicle (OMV) vaccine carries “several important” gonococcal antigens intended to prevent infection. Dr Jan Groen, CEO of Intravacc, hopes that the project will combine “our science and OMV expertise” in pursuit of an effective vaccine.
“We believe the outcome of this vaccine project could be an important contribution to the antimicrobial resistance epidemic.”
CARB-X takes on the drug-resistant challenge
CARB-X is developing a pipeline of “high-value products to prevent, diagnose, and treat bacterial infections that have become resistant to antibiotics”. Drug-resistant bacterial infections killed an estimated 1.27 million people in 2019.
“CARB-X emphasises performance characteristics that patients need against infections driving the greatest global morbidity and mortality.”
Since its establishment in 2016, CARB-X has supported 93 R&D projects in 12 countries, making “tremendous progress”. In 2022 new funding rounds were launched to support R&D projects and fill “critical gaps in the antibacterial pipeline”. Intravacc’s vaccine is the second project to receive a grant in the 2022-2023 funding call.
In December 2023 IAVI and Biofabri, a subsidiary of Zendal, announced that IAVI has been awarded US$55 million by the Bill & Melinda Gates Foundation to conduct a Phase IIb trial assessing the safety and efficacy of MTBVAC. MTBVAC is a tuberculosis (TB) vaccine candidate for the prevention of active TB lung disease in adolescents and adults. Thanks to an Open Philanthropy grant and additional funding from the German Federal Ministry of Education and Research (BMBF) the trial is expected to begin enrolling participants in mid 2024.
A historic opportunity secures funds
Dr Mark Feinberg, president and CEO of IAVI, is “thrilled to have secured the investment” that the team needs to advance the “promising vaccine candidate into an efficacy study”.
“The world urgently needs a new, effective vaccine that can prevent TB disease in adults and adolescents, and we are hopeful that MTBVAC will be part of the solution to finally end the TB epidemic.”
Dr Feinberg thanked the Bill & Melinda Gate Foundation for “their support”, also recognising Open Philanthropy, whose “visionary investment” could “accelerate the availability of MTBVAC by several years” if it proves safe and efficacious in trial. Dr Lewis Schrager is senior leader of TB vaccine development efforts at IAVI, describing this progress as an “historic opportunity”.
“If MTBVAC were shown to safely prevent TB disease in this population, this vaccine could prove to be critically important in global strategies to suppress the TB pandemic given its ease of use, low cost, and anticipated widespread availability.”
Dr Kundai Chinyenze, IAVI Africa director, is “gratified” to begin work on the trial in a region “where TB is a leading contributor to morbidity and mortality”, particularlly for people who are living with HIV.
“IAVI’s long history in conducting clinical trials in Africa and our strong network of regional and global partners provide a solid foundation for the successful conduct of this important trial.”
MTBVAC
The vaccine is being developed for two purposes: as a more effective and potentially longer-lasting vaccine for newborns, and for the prevention of TB disease in adults and adolescents. Previous Phase Ib/IIa dose-ranging studies in adults and neonates demonstrated “favourable immunogenicity and safety profiles”.
Designed by Dr Carlos Martín Montañés and Dr Brigitte Gicquel, MTBVAC was in-licensed by Biofabri. It is a live attenuated vaccine derived from Mycobacterium tuberculosis, the bacterium that causes TB disease in humans. It is the only live attenuated vaccine from this bacterium in the pipeline, and, with this derivation from the human TB-causing organism rather than the bovine, MTBVAC “has the potential to generate a broad protective immune response. Administrated via intradermal delivery, it does not require an adjuvant.
The study of MTBVAC to prevent TB disease is expected to enrol around 4,300 people who have latent TB infection in South Africa and “select other sub-Saharan African countries in areas with high TB burden”. They will be between the ages of 14 and 45. Over 15-20 trial sites the participants will receive a single dose of MTBVAC or placebo, with observation lasting two or three years.
Esteban Rodriguez, CEO of Biofabri, is “delighted by the fantastic opportunity” to evaluate the vaccine.
“The outcome of the efficacy studies in neonates as well as those in adolescents and adults will provide us with a pathway to license MTBVAC for all age groups.”
If the trial shows MTBVAC to be safe and efficacious, Biofabri, IAVI, and other collaborators emphasise their intention to “ensure” it is manufactured and supplied in “sufficient quantities globally” and is “accessible at affordable prices in low- and middle-income countries”.
Could this be the turning point in tackling TB? For more on exciting progress with vaccine development don’t forget to subscribe to our weekly newsletters here.
In December 2023 the PrEPVacc HIV prevention study announced that vaccinations in the study have stopped due to “little or no chance” that the trial will demosntrate vaccine efficacy in preventing HIV acquisition. PrEPVacc reports that the leadership team have responded to the recommendation of the independent data monitoring committee that vaccinations should stop but that the oral PrEP component of the study should “continue to completion”. Follow-up for all participants will continue for data collection, HIV testing, and referral for ongoing care for six months after the final vaccine injection for participants or until the end of the oral PrEP trial.
PrEPVacc
PrEPVacc is a “three trials in one” approach that is led by African researchers “with support from European scientists”. The goal is to test two HIV vaccine combinations to assess if either can prevent infection in populations that are at risk of acquiring HIV. Around 1,500 volunteers in East and Southern Africa were enrolled.
Participants received injections of a combination of a DNA vaccine with a protein-based vaccine (AIDSVAX), a regimen combining DNA, MVA, and a protein-based vaccine (CN54gp140), or a placebo. While the vaccinations were underway the trial also tested a new oral pre-exposure prophylaxis (PrEP) drug formulation to see if it is as effective as drugs that are already approved.
The recent statement reflects that “despite the delays experienced due to the COVID-19 pandemic”, all participants but 10 had passed the time point for the third set of vaccinations by 2nd October 2023, with 1,016 having received all four vaccinations. Almost all participants elected to receive oral PrEP. However, after a scheduled interim review on 9th November, which considered data collected up to 2nd October, vaccinations were stopped immediately.
HIV: high hurdles
“The stopping of further vaccinations in PrEPVacc underlines how challenging it is to develop an effective HIV vaccine.”
The trial results will be shared with the public after the completion of study visits and analysis in the second half of 2024. PrEPVacc’s Trial Director, Dr Eugene Ruzagira, announced the news at the International Conference on AIDS and STIs in Africa (ICASA) 2023.
“The scientific hurdles are high, but I have equally high hopes that an HIV vaccine will be developed one day. Every day, all around the world, important research like PrEPVacc is moving us forward, and participants are willing to step forward with us and make a difference to the health of their communities.”
Dr Ruzagira reflected that the study built “very good relations” with participants and communities through the “principles and techniques” of Good Participatory Practice.
“As we move forward towards a new era of HIV prevention studies and vaccine efficacy trials, the lessons Good Participatory Practice have never been more important to apply.”
Professor Pontiano Kaleebu is PrEPVacc’s Chief Investigator and emphasised that the development of a preventative HIV vaccine is a “critical goal for Africa”, which must “have even greater urgency now that no HIV vaccines are being trialled for efficacy anywhere in the world”.
“We have come so far in our HIV prevention journey, but we must look to a new generation of vaccine approaches and technology to take us forward again. We must also look to a new generation of leaders.”
Professor Kaleebu commended participants and collaborators on their contributions to the “largest HIV vaccine efficacy trial to run in East Africa”. Professor Jonathan Weber is from Imperial College London in the UK, sponsor of the trial, and agreed on the importance of thanking and crediting the participants, who have made “a tremendous ongoing commitment to this study”.
“Our participants’ willingness to continue this study with us is heroic and greatly appreciated by the research community.”
Reflecting that “we do clinical trials because we don’t know the answer”, Professor Weber reckons that the interim result “puts this generation of putative HIV vaccines to bed”.
“It has been a tremendous achievement.”
The trial is not over
Professor Sheena McCormack, Project Lead based in the UK, offered the reminder that the trial is “three studies in one, and the PrEP part is continuing”.
“We hope that we will have valuable insights from the quantitative and qualitative findings to guide the use of oral PrEP beyond the trial.”
Olivia Nakanwagi of the Community Advisory Board concluded the statement with a positive reflection that the trial has tried “new ways to bring the community’s voice into decision-making”.
“I’m proud to represent my community among the study leaders, scientists, and staff at my site and guide them in engaging well with that community.”
This last comment is particularly relevant considering the recent call from UNAIDS: “let communities lead”. If you haven’t yet read the report, you can access it through the article here. If this trial has put “to bed” a generation of vaccines, what does the future of HIV vaccine efforts hold?
In December 2023 VitriVax shared that the Bill and Melinda Gates Foundation has granted the organisation a two-year grant worth $5 million to support the further development of its proprietary single shot, thermostabilisation vaccine technology (ALTA). The funding will also enable the development of a pilot-scale manufacturing capacity.
VitriVax states that the project will focus on “formulation development, preclinical studies, and the development of Good Manufacturing Practice protocols to support future regulatory submissions.”
ALTA
We noted in July this year that VitriVax’s ALTA (Atomic Layering Thermostable Antigen and Adjuvant) technology platform has been engineered to enable thermostable, single-shot vaccines across multiple indications. VitriVax explains this technology in two parts:
Thermostability – a spray drying process embeds antigens and adjuvants in a sugar glass matrix to protect them against thermal and chemical degradation.
Single-shot administration – using Atomic Layer Deposition (ALD), the team applies nanometre-thick, precision coatings of protective metal oxides to the surface of antigen- and adjuvant-containing spray dried microparticles to provide timed release of doses up to 6 months after injection.
With the latest funding, the company will study the ALTA mechanism of action using model antigens, such as those that target HIV. VitriVax suggests that the platform is “highly scalable” and produces vaccines with “extended shelf life”, which will facilitate easier transportation and possible stockpiling.
Dr Romulo Colindres, CEO of VitriVax, is “honoured” by the Gates Foundation’s support of VitriVax’s “efforts to advance equitable access to vaccines around the world”.
“VitriVax, with funding from the Bill and Melinda Gates Foundation, is taking an important step forward in establishing its vaccine technology.”
In 1988 the first World AIDS Day was launched under the theme “A world united against AIDS”; in 2023 the global health community continues to observe it, calling “let communities lead” in the UNAIDS Report 2023. WHO describes World AIDS Day as an opportunity to “reflect on progress”, to “raise awareness”, and to “mobilise all stakeholders” in efforts to “ensure the success of the HIV response”. UNAIDS states that the day allows everyone to participate in campaigns around “specific themes related to HIV”:
Awareness-raising activities take place around the globe
People can wear a red ribbon, the universal symbol of awareness of, support for, and solidarity with people living with HIV
People living with HIV make their voices heard on issues important in their lives
Groups of people living with HIV and other civil society organisation involved in the AIDs response mobilise in support of the communities they serve and to raise funds
Events highlight the current state of the epidemic and global response
In this article we examine the report and its implications for the vaccine community in particular; we invite you to share your insights or experience for World AIDS Day 2023.
A call for communities
In the foreword by Executive Director Winnie Byanyima a sobering statistic is stated:
“Every minute, a life is lost to AIDS.”
Despite significant advances in the global response, 9.2 million people with HIV are unable to access life-saving antiretroviral therapy. Every week, 4,000 women and girls become infected with HIV. However, for Ms Byanyima this is “not fate”. Reflecting on the role of communities, she states that we can end AIDS as a public health threat by 2030.
The report is both a celebration of community involvement and a “call to action” to decision-makers, demanding that they empower communities and reduce barriers to community leadership as outlined in the press release:
Communities’ leadership roles should be made core in all HIV plans and programmes
Communities’ leadership roles should be fully and reliably funded
Barriers to communities’ leadership roles should be removed
“Communities are not in the way – they light the way to the end of AIDS. Let communities lead!”
The report
UNAIDS sets an example of community engagement by featuring nine guest essays in the report, each exploring personal experiences of achievements, barriers, and ambitions. Alongside these essays are examples of communities driving innovation and demanding appropriate services. The report suggests that, despite agreeing on targets, the world has “yet to follow through”.
There remains a “host of barriers” to community-led responses, but the report helpfully presents “three vital lessons”:
AIDS can be ended as a public health threat with communities leading the way. Communities deliver essential HIV and sexual and reproductive health and rights services that accessible, grounded in community needs, and able to reach the most marginalised people. Communities have an ability to advocate necessary policy change and serve as accountability watchdogs. Although community-led responses drive progress in all aspects of the HIV response, the role of community will be critical in traversing the final mile and sustaining gains beyond 2030.
“No other actor can deliver what communities can.”
The path to ending the AIDS pandemic is obstructed by the restraining of communities’ leadership roles. However, the issue is not just a capacity issue – communities have the knowledge, innovation, and solidarity that is needed to transform national HIV responses.
“They are often blocked from fully leveraging this capacity.”
The barriers to communities’ leadership roles can be removed, which is in the power of authorities such as national governments, donors, and other stakeholders. This means providing community-led organisations with the resources they need, such as core funding. Furthermore, it means recognising that communities are not in the way. Governments must ensure safe and meaningful space to allow communities to do their essential work, removing punitive laws and policy barriers.
The report delivers a message of “active hope”, recognising that, although the world is “not currently on track to end AIDS as a public health threat”, it can “get on track”.
“For the HIV response to succeed, let communities lead!”
Communities and access to medicine
One area of the report that stands out as pertinent to the vaccine community is the section on affordability of HIV medicines. It suggests that during the HIV “treatment revolution” in the “mid-1990s”, antiretroviral therapy combinations “rapidly transformed HIV from an invariably fatal disease” to a “chronic and manageable” disease. Unfortunately, this change was almost exclusively experienced by people in high-income countries.
“This inequality echoed what had been experience in many other health challenges, in which many years and sometimes several decades were required for the prices of medical innovations to decline sufficiently to enable meaningful uptake in resource-limited settings.”
The report indicates that it was communities who “insisted” that this approach was not to be tolerated, undertaking global, regional, and country level advocacy, pursuing strategic litigation, and engaging with trade and intellectual property processes. The result was a “cascade of actions” that reduced the annual per-person cost of antiretroviral therapy by more than 99%: from US$ 10,000 in 2000 to less than US$50 for the recommended first-line regimen in 2023.
This year, community-led advocacy “contributed to another landmark advance” in the effort for “affordable, universally accessible medicines”; the Government of Colombia decided to list dolutegravir as a medicine of public interest, enabling the purchase of generic versions.
Responding to this section of the report, we are reminded of our interview with Dr Gaurav Gaiha in Washington this year. We know that HIV therapy is a lifelong and challenging aspect of the lives of people living with HIV, so we asked how a vaccine could overcome these issues. Dr Gaiha reflected that, not only would a preventative vaccine be “fantastic”, but a therapeutic vaccine that could “suppress the virus” would be a “huge development”.
“HIV is one of those viruses where vaccine development is very much in line with addressing this issue of access.”
Another of our previous interviews that covers HIV vaccines was with Dr Mark Feinberg, who described HIV as “the most vexing pathogen” that vaccinologists are tackling. His focus in the diseases that had been “forgotten” during the COVID-19 pandemic invites us to consider the diversion of resources that may have happened, and how a ‘catch-up’ can be achieved. He was emphatic that these diseases were not “forgotten” by the people who experience them, and this relates back to the importance of communities and their role in driving innovation and investment.
What does the report demand?
The conclusion emphasises that communities must be kept central to progress.
“The historic achievements the world has made in the HIV response have been possible only because of visionary courageous leadership and action by communities.”
“Communities do not lack commitment, knowledge, or insights, but they do lack the full, unstinting support they need to accelerate progress towards ending AIDS.”
Therefore, the report demands “sufficient resources” and optimal engagement in decision-making. In some countries, community leadership is “compromised by a repressive legal environment and a restrictive space for civil society”. This “treats communities as a problem to be managed” instead of the solution. Finally, the report authors are explicit as they state that the intended audience of their guidance is not the communities, but the governments, donors, and stakeholders who need to “act now, with boldness”.
Community responses to the report
UNAIDS’ statement shares comments from various advocates and community members. Quoted is Robbie Lawlor, Co-Founder of Access to Medicines Ireland, who states that “We are the vehicle for change that can end systematic injustices that continue to fuel HIV transmission”.
“Yet, we are expected to move mountains without being financially supported. We are supposed to fight for a more equitable world and are tasked with dismantling stigma yet are side-lined in crucial discussions. We are at a tipping point. Communities can no longer be relegated to the periphery. The time for leadership is now.”
Minister of State for Development and Africa in the UK, Andrew Mitchell, is “extremely concerned about the exclusion from health services of key populations like the LGBT+ community”. He thanked UNAIDS for “keeping us focused on the inequities” that drive the pandemic and looked forward to collaborating to “champion the voice of people living with HIV” and “end AIDS as a public health threat by 2030”.
Solange Baptiste is Executive Director of the International Treatment Preparedness Coalition and reflects that “community-led action” is the “most important countermeasure” in the AIDS response.
“Yet, shockingly, it isn’t a cornerstone of global plans, agendas, strategies, or financing mechanisms for improving pandemic preparedness and health for all. It is time to change that.”
If you’ve read the report, do let us know what you found most significant or helpful, and share how you might translate this into action!
In November 2023 the UKHSA and University of Bristol shared a report that reveals the results of an NHS England emergency department opt-out testing programme. The report was commissioned by NHS England to evaluate the first year of the programme, which tests for bloodborne viruses. It tests people in emergency departments who are having a blood test, regardless of symptoms. UKHSA states that this programme will increase diagnoses and treatment for HIV, hepatitis B, and hepatitis C, supporting elimination goals.
Testing for BBV
In April 2022 an NHS England funded programme of testing for bloodborne viruses (BBVs) in emergency departments (EDs) began. This was focused in “areas of very high diagnosed HIV prevalence” (5 or more people per 1,000 people between the ages of 15 and 59). Across 33 EDs 857,117 HIV tests, 473,723 hepatitis C virus (HCV) tests, and 366,722 hepatitis B virus (HBV) tests were conducted during the first year.
“The scale of the programme makes it a substantial contribution to all BBV testing in England.”
The report offers an interim public health evaluation from the first 12 months of the programme. Dr Sema Mandal, Deputy Director of Blood Safety, Hepatitis, STI, and HIV division at UKHSA, believes that the programme has already had a “significant” effect. The report “highlights how many people are living with an undiagnosed bloodborne virus.”
“Fewer new diagnoses of HIV and hepatitis C were made compared to hepatitis B, highlighting the significant efforts and financial investment made to enhance diagnosis and treatment for HIV and HCV. Similar efforts are necessary for HBV to meet disease elimination targets.”
Interim recommendations
The following recommendations are offered.
Delivery of testing:
Develop and implement standard operating procedures (SOPs) for opt-out testing for all BBVs if these are not yet in place and ensure ED staff are fully briefed.
Adopt opt-out procedures recommended as good practice, using verbal prompts where appropriate.
Continue to work with electronic patient record (EPR) teams in sites that do not yet have automated test ordering in place to replicate approaches taken by other sites with high uptake.
Develop procedures to contact individuals in the event of insufficient blood samples and to inform individuals if no BBV test has been performed.
Continue to work with sites with low test uptake to understand barriers to testing and to facilitate higher testing rates.
Linkage to care:
Map and optimise care pathways for people newly diagnosed with HBV in ED as part of roll out of ED testing to new sites.
Continue to improve linkage to care from ED by identifying the needs of individuals diagnosed in ED and structural facilitators to linkage to care, including additional interventions such as community support.
Continue to share learning from different care pathways used within the programme.
Evaluation and surveillance:
Collaborate to increase recruitment of laboratories to SSBBV to improve representative coverage across sites, including those outside London.
Work with laboratories to understand and address data incompleteness and recording of ED test setting SSBBV surveillance data.
Investigate ways to identify confirmatory testing for HIV in SSBBV surveillance data.
Undertake a deep dive with selected sites to understand why some people with positive HIV results are not matching to HARS and are not categorised as ED test setting.
Work with HIV and sexual health clinics to improve recording of first site of HIV test to better understand the extent of ED testing nationally.
Encourage sites to work with UKHSA on monitoring HBV linkage to care.
What does the report conclude?
The report states that the programme has demonstrated that opt-out ED BBV testing “can be delivered at scale” and “equitably”, despite large differences between sites. Although the programme has not yet reached the target of 95% of eligible people being tested, the data represent early stages.
Identified issues include the confusion caused by a “no news is good news” approach, where individuals might assume that they have been tested. Therefore, sites are encouraged to develop procedures to “mitigate this risk”. The programme was “effective” at identifying new diagnoses for all 3 BBVs, the highest number being HBV. This high number has “implications of how to meet the increased need for HBV care when considering expansion”. Linkage to care is described as “sub-optimal” for all 3 BBVs, but more so for HBV and HCV than HIV.
“There were limitations in the coverage and completeness of surveillance data for this evaluation.”
Making contact count
Matt Fagg, NHS England’s director for prevention and long-term conditions, said that “thanks to our routine opt-out testing programme” the NHS has been able to “identify and treat thousands more people” living with HIV and hepatitis.
“Without this testing programme, these people may have gone undiagnosed for years, but they now have access to the latest and most effective life-saving medication.”
The NHS, he says, is “committed to making all contact with patients count”. Public Health Minister Neil O’Brien agrees that the “amazing programme” is already making a “real difference”. He is “grateful” to the NHS for its “excellent work”. Professor Kevin Fenton, Chief Advisor on HIV and Chair of the HIV Action Plan Implementation Steering Group reflected that the “flagship initiative” is effective in “identifying people living with undiagnosed HIV” so they can be “signposted to support and treatment”.
“While we know there are improvements to be made, this data gives us confidence that this essential part of our strategy is working. It’s crucial that we continue scaling up HIV testing, so people receive high quality care as we work towards ending HIV transmission in England by 2030.”
Detecting silent threats
Pamela Healy, Chief Executive of the British Liver Trust, described hepatitis B as an often “silent virus” with “thousands of people” in the UK unaware that they have it. If this virus is left undetected, it can cause liver damage or increase the risk of liver cancer.
“It is crucial to find and provide treatment to these people to stop the virus causing further health issues and transmission.”
Daniel Fluskey, Director of Policy at National AIDS Trust, suggests that “at least 340 people” who now know they are living with HIV can “access transformative treatment”. He encourages the NHS to take the “vital” lessons from the evidence to ensure that more people get diagnosed.
Expansion plans
Rachel Halford, The Hepatitis C Trust Chief Executive, commented that the pilot scheme has proven to be a “successful way to find people” who are living with HIV, hepatitis B, or hepatitis C. She offers the example of people who are experiencing homelessness and “only interact with healthcare services via emergency departments”. This scheme is a “great way to reach and treat these people”.
“This life-saving initiative must now be expanded across the whole of the UK to ensure that everyone who is living with a bloodborne virus is found and offered treatment.”
Anne Aslett, CEO at Elton John AIDS Foundation, reflected that “opt-out HIV testing works to diagnose HIV and find those who have dropped out of care” due to “stigma and other challenges facing treatment”. However, there are still 4,400 people who live with undiagnosed HIV, she suggests.
“We need to ensure that we reach all communities across the country and roll out this successful method of HIV diagnosis to other high prevalence areas.”
Richard Angell, Chief Executive of Terrence Higgins Trust, agrees.
“It’s now time to urgently expand opt-out to more A&Es in England to change even more lives and ensure we make the rapid progress necessary to end new HIV cases by 2030.”
In November 2023 the UK’s Joint Committee on Vaccination and Immunisation issued advice to the government on a routine targeted vaccination programme for the prevention of gonorrhoea alongside advice on a routine vaccination programme against mpox for those at greatest risk. JCVI recommends that both programmes should be offered on an “opportunistic” basis through specialist sexual health services with experience in assessment and identification of people at increased risk of infection with bacterial STIs. The UKHSA and Department of Health and Social Care state that ministers will consider the advice before making policy decisions.
Gonorrhoea
The JCVI states that gonorrhoea is a bacterial STI caused by the Neisseria gonorrhoeabacterium and is the “second most commonly diagnosed” STI in England; around 80,000 cases are diagnosed a year. It is transmitted through unprotected anal, oral, or vaginal sex, or genital contact with an infected partner. People who are infected may not display symptoms but can still transmit infection.
“Typical” symptoms include thick green or yellow discharge from the vagina or penis, and painful urination. The infection can also cause pelvic inflammatory disease, ectopic pregnancy and infertility, or painful infection in the testicles and prostate.
“Gonorrhoea causes significant morbidity and remains a public health concern globally.”
This concern increases as resistance to antibiotics increases; WHO considers the pathogen a priority pathogen due to the widespread antimicrobial resistance. In the UK, the recommended first-line therapy is ceftriaxone, to which resistance remains “very low”. However, resistance is increasing.
The UK has been conducting surveillance for “over 100” years, and the number of diagnoses in 2022 was the “highest annual number on record”. These rates are “consistently disproportionately higher” in “specific communities”. These include:
Those who live in the most deprived areas
People of black Caribbean ethnicity
People born in Central or South America (this measure is used as a proxy for being of Latino, Latina, or Latine ethnicity)
Young people 15-24 years old and gay, bisexual, and other men who have sex with men (GBMSM)
“Natural infection does not give protection against future infections, and among both GBMSM and heterosexuals, a recent history of gonorrhoea is a reliable predictor of future reinfection with gonorrhoea or other STIs.”
JCVI’s recommendation
The latest advice suggests that a targeted vaccination programme should use the 4CMenB vaccine to prevent gonorrhoea. It is a 4-component serogroup B meningococcal vaccine containing:
3 main Neisseria meningitidis proteins
Neisseria heparin binding antigen (NHBA)
Neisserial adhesion A (NadA)
Factor H binding protein (fHbp)
Meningococcal serogroup B outer membrane vesicles (OMVs)
There is one licensed 4-component vaccine in the UK: Bexsero. This is manufactured by GSK and authorised for the prevention of meningococcal disease in patients over the age of 2 months. It’s used in the routine childhood programme administered at 8 weeks, 16 weeks, and 1 year for the prevention of meningococcal disease.
“Neisseria meningitidis and Neisseria gonorrhoeae are closely genetically related with between 80 to 90% sequence homology. This homology gives the potential for cross-protection from OMV containing meningococcal B vaccines against Neisseria gonorrhoeae.”
The JCVI agreed that the targeted programme should be “initiated” using the 4CMenB vaccine for gonorrhoea prevention in those who are “at greatest risk”. It emphasises that individuals who are offered vaccination must understand that real world studies have estimated that the vaccine has “between 32.7% to 42% effectiveness against gonorrhoea”. Therefore, although it would “be expected to reduce the chance of becoming infected”, it would “not completely eliminate the possibility”.
“Vaccinated individuals could expect to have some reduction in their own risk of contracting gonorrhoea; however, the main benefit of a vaccination programme is expected to be at a community level.”
Professor Andrew Pollard, Chair of the JCVI, hopes that the programme would not only “be a world first” but “should significantly help to reduce levels of gonorrhoea, which are currently at a record high”. Dr Katy Sinka, Head of Sexually Transmitted Infections at UKHSA, described a vaccination programme that would reduce gonorrhoea cases as a “hugely welcome intervention”.
“We saw a rapid rise last year with more cases than ever before and with gonorrhoea becoming increasingly resistant to antibiotics, tackling this infection is a serious concern.”
Mpox
Mpox (previously called monkeypox) is a “rare disease caused by infection with the mpox virus”, an orthopox virus related to the viruses that cause smallpox and cowpox. JCVI states that before early 2022, cases of mpox in the UK were “either associated with travel to or from countries where mpox is endemic”. However, in May 2022 there was a “large outbreak” in the UK that presented a “different” pattern and scale to what had previously been observed.
During this outbreak, cases were “primarily identified among gay, bisexual, and other men who have sex with men” (GBMSM) without a history of travel to endemic countries. From this it was inferred that there was community transmission; epidemiological surveillance suggested that this occurred from person-to-person contact in “defined sexual networks of GBMSM”.
In response, although there was no licensed vaccine for protection against mpox, there was “good evidence” that the Modified Vaccinia Ankara – Bavarian Nordic (MVA-BN) provided cross-protection to mpox when given pre-exposure. The MHRA approved this vaccine for immunisation against mpox in September 2022. However, due to a limited supply of vaccines, intial recommendations focused on first doses.
JCVI’s recommendation
For mpox, the JCVI advises an “ongoing routine vaccination strategy” to prevent outbreaks and protect those at risk of exposure. This advice encourages the strategy to “target GBMSM who are at highest risk of exposure”; they will be identified via sexual health services through “markers of high-risk behaviour” such as those used to assess eligibility for HIV pre-exposure prophylaxis (PrEP). These criteria include:
A recent history of multiple partners
Participating in group sex
Attending sex-on-premises venues
A proxy marker such as a bacterial STI within the last year
Furthermore, JCVI encourages efforts to “ensure” that the vaccine is “offered equitably to those at equivalent risk”, including “transgender women or gender-diverse people assigned male at birth”. Dr Sinka commented that “while mpox case numbers across England remain very low” the community should “not be complacent”.
“Any routine vaccination offer to those at highest risk of infection will help ensure we remain on top of the disease and prevent any major future outbreaks.”
Updates to the latest advice are expected as further information about “vaccine effectiveness and duration of protection” becomes available.
How might these recommendations influence policy for better infection control in the UK, and can we expect to see other areas follow this decision? If your country has a better approach to infection management, why not share it? For more on vaccination policy and practice don’t forget to subscribe here.
In November 2023 the WHO shared the Global Tuberculosis Report 2023, a “comprehensive and up-to-date assessment” on the epidemic and progress in preventing, diagnosing, and treating the disease at all levels. The report uses data from national ministries of health, with 192 countries and areas providing insights into more than 99% of the global population and cases. WHO reflects that the report “underscores a significant worldwide recovery” from 2022, an “encouraging trend” in response to the “detrimental effects of COVID-19 disruptions” on tuberculosis measures.
The ‘what’ and ‘why’
The report begins with an introduction to this “preventable and usually curable disease”: tuberculosis (TB). It is caused by the bacillus Mycobacterium tuberculosis, spread through bacteria expelled into the air by infected patients. Despite the progress that has been made in prevention and control, WHO reports that, in 2022, TB was the “world’s second leading cause of death from a single infectious agent”, following COVID-19. It caused “almost twice as many deaths as HIV/AIDS”.
“More than 10 million people continue to fall ill with TB every year.”
Roughly quarter of the global population is believed to have been infected with TB, and the risk of developing TB disease is highest in the first 2 years after infection. However, some may clear the infection. Although the disease “typically affects the lungs”, it can affect other areas as well. If a patient cannot access treatment, the risk of death is high, but for those who receive the recommended 4–6-month course of anti-TB drugs, there is an 85% chance of curing it.
“Universal health coverage (UHC) is necessary to ensure that all people who need treatment for TB disease or infection can access these treatments.”
The report also states that the number of people who become infected and develop disease, and consequently the number of TB-related deaths, can be reduced through “multisectoral action” to address determinants such as “poverty, undernourishment, HIV infection, smoking, and diabetes”. Despite these management strategies, WHO calls for “research breakthroughs” such as a new vaccine to “rapidly reduce” TB incidence.
In September 2023, a high-level meeting on TB resulted in a political declaration that “reaffirms” global targets. This report, just over a month later, comprises 3 components. The main report presents “key findings and messages”, which we explore below. To access the report yourself, click here.
Main findings and messages
The report offers an optimistic indication that we have seen “major global recovery” in the number of diagnoses and patients treated after 2 years of “COVID-related disruptions”. Although this has “started to reverse or moderate” the effects of the pandemic on the number of people dying or experiencing illness with TB, the disease was still second to COVID-19 as the cause of death from a single infectious agent. While there is a positive trend, global targets set in 2018 “have been missed” and others remain “off track”.
Case notifications
The “most obvious and immediate” consequence of COVID-19 on TB was a “large global fall” in the number of people who were “newly diagnosed with TB and reported”. Between 2019 and 2020 there was a reduction of 18%, from 7.1 million to 5.8 million, with a “partial recovery” to 6.4 million in 2021. In 2022, 7.5 million people were newly diagnosed and officially notified as a TB case, a “rebound” to above the pre-COVID-19 level that “probably” reflects the diagnosis of a “sizeable backlog of people” as well as an increase in cases.
Deaths caused
The report infers from the reduction in reported cases that “the number of people with undiagnosed and untreated TB had grown”. This means that there was an increase in deaths from TB and more community transmission of infection, which later results in increased numbers of people developing TB. In 2022 the total number of deaths caused by TB was 1.30 million, which is down from “best estimates of 1.4 million in 2020 and 2021”. COVID-related disruptions are estimated to have resulted in “almost half a million excess deaths from TB” between 2020 and 2022, compared to the number if pre-pandemic trends had continued.
Number of people developing TB
In 2022 an estimated 10.6 million people became ill with TB, an increase from 10.3 million in 2021 and 10.0 million in 2020. The TB incidence rate (new cases per 100,000 population per year) is believed to have increased by 3.9% between 2020 and 2022. This comes after an average decline of about 2% a year from 2010 to 2020. The subsequent “reversal of progress” reflects the estimated effect of disruptions to essential services during the pandemic/
Milestones
This finding contrasts “some success stories” at regional level with a “mostly off track” warning. The first End TB Strategy milestones for reductions in TB disease burden were a 35% reduction in total deaths and a 20% reduction in TB incidence rate by 2020, in comparison with 2015. The second milestones were set for 2025: a 75% reduction in deaths and a 50% reduction in incidence.
“The first milestones set for 2020 have not yet been reached either globally or in most WHO regions and countries, and the second milestones are far away in most parts of the world.”
Beyond 2022
The report refers to 26 country-specific models for the period of 2020-2022, which also allow projections for subsequent years. It is hoped that if the recoveries in 2022 are sustained, the global number of deaths should “continue to decline”. The upward trend in TB incidence may be reversed in 2023 or 2024.
Global targets can only be achieved if diagnostic, treatment, and prevention services are offered “within the context of progress towards UHC” with “multisectoral action to address the broader determinants”. When countries adopt the Sustainable Development Goals (SDGs), they commit to achieving UHC by 2030.
The need for a vaccine
The End TB Strategy targets will not be met without “intensified research and innovation”. The priorities identified in the report include a “vaccine to reduce the risk of infection” and a vaccine or drug to “cut the risk of TB disease in people already infected”. In 2020 Member States adopted WHO’s strategy for research and innovation, which seeks to encourage “accelerated” research and innovation and “improve equitable access” to the results of this research.
Despite some progress, research is “constrained by the overall level of investment”. Although WHO recognises “modest increases”, recent data show that only “half of the global target” from the first high-level meeting on TB has been secured.
Dr Tedros Adhanom Ghebreyesus, WHO Director-General, commented that humanity has the “opportunity that no generation in the history of humanity has had: the opportunity to write the final chapter in the story of TB”.
An artificial intelligence (AI) tool developed by a team from the University of Oxford and Harvard Medical School could help predict new viral variants according to findings in Nature in October 2023. The University of Oxford reports that EVEscape, the model, predicts the likelihood that a viral mutation will enable it to “escape immune responses”. EVEscape combines three sources of information to “score” individual mutations:
A deep generative model for fitness protection
Structural information about the spike protein to estimate antibody binding potential
Chemical distances in charge and hydrophobicity between mutated and wild type residues
COVID-19
The research paper states that “extensive surveillance sequencing and experimentation” from the COVID-19 pandemic have presented a “unique opportunity” to assess EVEscape’s ability to “predict immune evasion” before escape mutations are observed.
“The ability of EVEscape to identify the most immunogenic domains of viral proteins without knowledge of specific antibodies or their epitopes could provide crucial information for early development of subunit vaccines in an emerging pandemic.”
Contributing author Associate Professor Yarin Gal believes that the “critical aspect” to the team’s approach is the methods “do not have to wait for relevant antibodies to arise in the population”. DPhil student and co-lead author of the study Pascal Notin commented that “had EVEscape been deployed at the start of the COVID-19 pandemic, it would have accurately predicted the most frequent mutations and the most concerning variants for SARS-CoV-2″.
The study evaluated the model’s ability to make early predictions based on the limited information available at the start of the pandemic. It was able to successfully predict emerging and prevalent mutations as well as which antibody-based therapies would lose efficacy. EVEscape was also effective at predicting immune escape mutations for influenza, HIV, and “understudied viruses with pandemic potential” like Lassa and Nipah.
Vaccine design
The work represents a huge advance in disease control, and Notin suggests that it has “tremendous value” for pandemic surveillance and vaccine design.
“The most exciting next step for this line of work is demonstrating how it can be used in practice to inform vaccine design.”
Associate Professor Gal agreed that “anticipating viral variants that avoid immune detection with sufficient lead time” will be ‘key to developing optimal vaccines and therapeutics”.
“Antibody escape mutations affect viral reinfection rates and the duration of vaccine efficacy.”
In October 2023 the University of Oxford’s Oxford Vaccine Group announced funding from the Medical Research Council within UK Research and Innovation (UKRI) to support a “pioneering” study into human immunity. The study is called LEGACY03 and will investigate how lymph nodes work and contribute to vaccine responses in patients of different ages. This research will potentially inform vaccine design for different age groups.
LEGACY03
The study is open to participation from volunteers between the ages of 18 and 45 and over the age of 65. It will take place at the Churchill Hospital’s Centre for Clinical Vaccinology and Tropical Medicine. Participants will be enrolled for 3 months, with the results supporting better vaccine design for “different age groups throughout life”. Participants will be given two licensed vaccines: an mRNA COVID-19 booster vaccine and a seasonal flu jab.
“As we age, our immune system changes and with it our response to vaccines. Our risk of complications from infections like flu and COVID-19 also increases and it is therefore important to understand these changes so that vaccinations can be better tailored for maximum efficacy to protect the most vulnerable.”
Dr Katrina Pollock, MRC Clinician Scientist in Vaccinology at the Oxford Vaccine Group, Department of Paediatrics, was “keen to improve understanding of the immune system” and respond to the “challenges in adult vaccinology”, which she suggests are “two-fold”.
“The first major challenge is the diversity of responses to vaccines in different people, particularly the most vulnerable like older adults or those living with conditions that affect the immune function. The second major challenge is making vaccines for targets that rapidly evolve, like COVID-19 and HIV.”
Dr Pollock states that the study will “take an innovative look” at individual immune responses, investigating human immunity “at the cellular level”.
“This will help us to tailor future vaccine design to get a better outcome for patients across the board. It has the potential to impact patients for the better and that is what drives my research.”
Lymph nodes
Lymph nodes are “small bean shaped organs” that can be found all over the body. When a vaccine is administered, white blood cells transport some of the vaccine back to the lymph nodes for a response to happen. In this study, the lymph nodes will be visualised with an ultrasound scanner and cells extracted to understand how they are responding. The cells will be sampled using the “safe and well-tolerated” technique, fine needle aspiration (FNA).
A commentary in The Lancetin October 2023 calls for a “gender-responsive” Pandemic Accord to secure a “healthier, equitable future”. The need for a Pandemic Accord was established by WHO’s Member States after the “impact” of the COVID-19 pandemic. WHO states that the proposed accord will be driven by a focus on “equity” in both “access to the tools needed to prevent pandemics” and “access to health care for all people”. However, the article suggests that “despite widespread advocacy”, governments and health leaders are failing to apply a “systematic intersectional gender lens” to negotiations.
Disease and gender
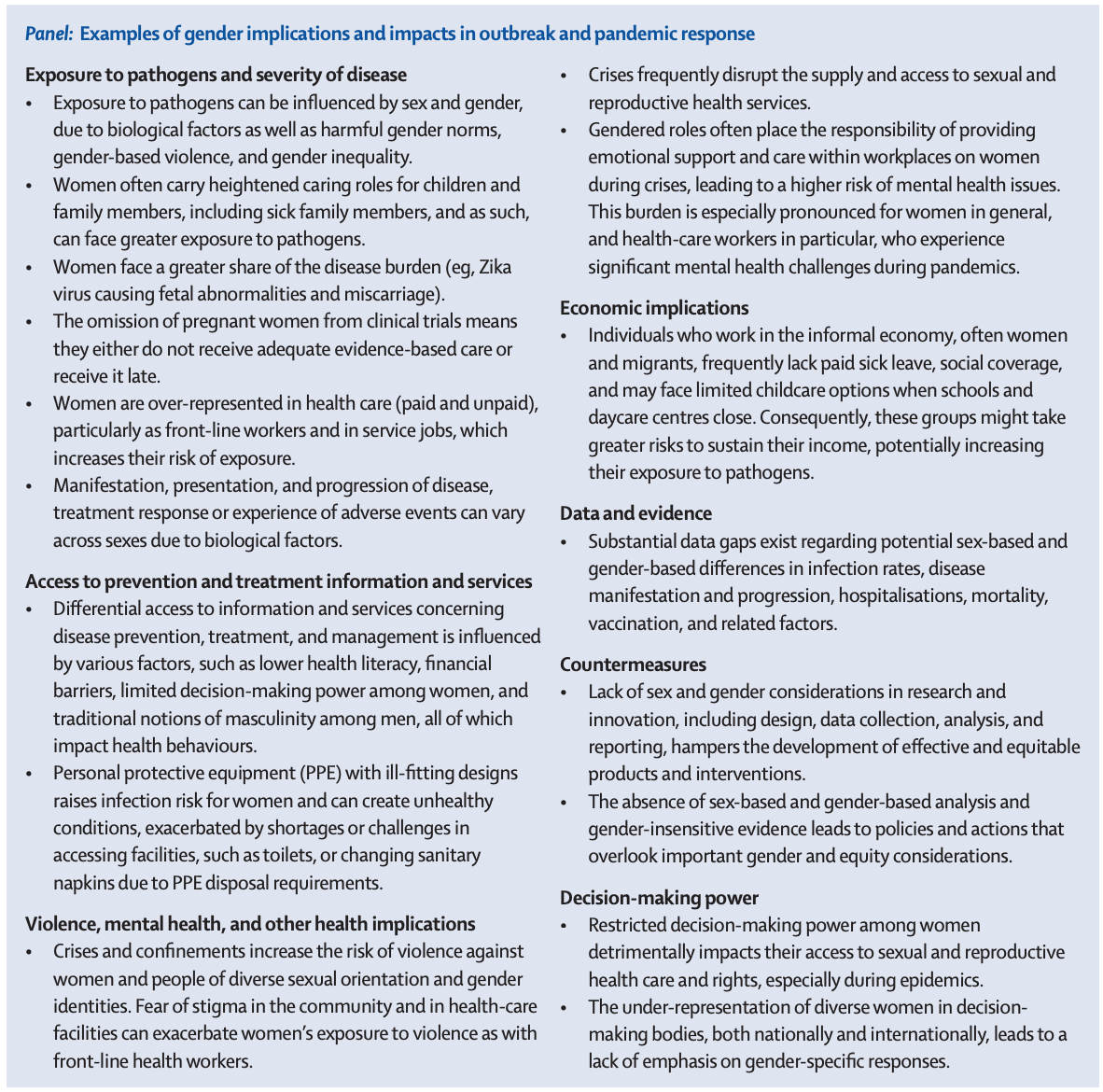
The article states that multiple diseases, from HIV and influenza to our recent experience of the global COVID-19 pandemic, have highlighted the “gender implications of disease outbreaks”. Furthermore, the lack of a gender lens in epidemic responses has documented “detrimental effects”, as demonstrated in the figure below.
“Pandemics create differential vulnerabilities with particular negative implications for women in all their diversities and their health, and further exacerbate long-existing, deep-rooted gender inequalities and social injustices, more severely disadvantaging women in low-income and middle-income countries, women in marginalised communities, and women who are criminalised.”
The authors suggest that a “massive data gap” exists around sex and gender differences in infection rates, hospitalisations, morbidities, and deaths, as well as the uptake in vaccines or how effective countermeasures have been. WHO is reportedly committed to “systematically collect, analyse, and report sex-disaggregated and gender data and embed them in policy making and programme design”. Despite this, there is “insufficient availability of sex-disaggregated data” for “most of the relevant Sustainable Development Goal indicators”.
Furthermore, post-COVID-19 investigations have “paid scant attention” to the effects of intersectionality, which puts us at a “high risk” of “not embedding gender and equity considerations” into future preparedness or response efforts.
“We are at a crucial juncture: a globally binding international health instrument with long-lasting effects on future responses to public health emergencies is being negotiated in the midst of a polarising global health environment, where sexual and reproductive health and rights are under siege and women’s rights and those of people of diverse sexual orientation and gender identities are infringed and retracted.”
Concrete measures
The authors demand “concrete measures” to ensure that gender-related concerns do not “fall by the wayside” in future pandemic preparedness and response. They refer to “irrefutable evidence” that a “gender, equity, and human rights lens” brings positive and sustainable effects to health and development. Despite this evidence, we need “political will” to learn lessons and recognise the “crucial need and value” of “embedding gender as an integral and cross-cutting theme” in the Pandemic Accord.
Highlighted in the paper are “key areas” that have so far been overlooked.
Key areas
Binding commitments – needed for generating sex-disaggregated data and gender responsive evidence to guide pandemic preparedness, control, and response. Within this, investment into data systems and research processes is imperative.
Inclusive, equitable strategies, policies, and response plans that account for gender dimensions and align with human rights standard – efforts to prevent discrimination and violation of rights of marginalised groups should be scaled up. Language guaranteeing uninterrupted access to health services and prevention of and adequate response to gender-based violence should be explicit. New policies should be effectively designed to be gender transformative, address harmful norms, and strive to eliminate the root cause of gender inequality.
Participation of diverse groups in the Pandemic Accord development – effective measures result from inclusive, consultative, transparent, and participatory decision-making processes that consider the needs and perspectives of different groups. The Pandemic Accord and interim medical countermeasures platform have the potential to shape a more equitable global health agenda.
“Today, the global community stands at an open window of opportunity – a chance to show future generations that lessons learnt from the past have inspired bold steps to enshrine gender equity to shape a healthier and fairer world for all.”
How do you think these suggestions could be practically implemented within the Pandemic Accord and in subsequent global health strategies?
In September 2023 Revital Healthcare announced a “historic milestone in African manufacturing excellence”. The company was awarded Pre-Qualification (PQ) status by WHO in July 2023 for its early activation auto-disable (AD) syringe in Africa. This marks more than 10 years of commitment to injection safety in immunisation programming across Africa.
Early activation
The early activation feature is described as the “gold standard for safety in immunisation programmes”. It disables the syringe at the start of administration and injection. These devices have caused a substantial reduction in rates of blood-borne infections like HIV in immunisation programmes across Africa.
A milestone to celebrate
Although 8 manufacturers have WHO PQ status for the product, Revital is the “first and only” that is produced in Africa. This is expected to decrease average syringe transport times by up to 90%. Director of Marketing and Sales for Revital is Roneek Vora, who comments on the “historic” prequalification. This “exemplifies the transformative power of African innovation and manufacturing excellence”.
“Our commitment to the well-being of fellow people, especially children receiving life-saving immunisation, is our motivation to continue to progress.”
Gates Foundation support
Revital suggests that it will be able to produce “upwards of 300 million AD syringes every year”. This is supported by a grant from the Bill and Melinda Gates Foundation. Not only does the grant contribute towards the development of the product, but it created more than 200 local jobs in Kilifi County. Of these new roles, 80% have been assumed by women in “support of a joint commitment to gender equality”.
Violaine Mitchell, Director of Immunisation at the Gates Foundation, is “proud to support Revital’s efforts” to “sustainably expand the supply of these syringes”.
“As the first African manufacturer to be approved by WHO to produce early activation auto-disable syringes, Revital is paving the way to expand local production of syringes.”
An article in Vaccine: X in August 2023 acknowledges that previous research has identified religion as one of “numerous factors” contributing to a potential delay or refusal of vaccination. Therefore, the author, PhD candidate Hanne Amanda Trangerud of the University of Oslo, seeks to present a “comprehensive overview” of the “essence” of religious objections to vaccination. This could be used to inform vaccination strategies with a greater understanding of vaccine decision-making. Trangerud offers five main types in the typology:
A worldview clash type – in which vaccines do not make sense as a health intervention
A divine will type – which represents a form of passive fatalism
An immorality type – which considers vaccines unethical because of their production or effect
An impurity type – pointing to ingredients that will defile the body
A conspiracy type – in which a vaccine plot is targeting a religious group
Vaccine decision-making and religion
“Vaccine hesitancy refers to delay in acceptance or refusal of vaccines despite availability of vaccine services. Vaccine hesitancy is complex and context specific, varying across time, place, and vaccines. It is influenced by factors such as complacency, convenience, and confidence.”
In a previous post we have explored the 5c model that examines these factors and more. It is important to note that vaccine hesitancy is distinct from low immunisation coverage due to supply and delivery. The notion of vaccine hesitancy as behaviour has been challenged by some, who argue that it should be understood as a “state of indecisiveness”. However, for Trangerud, the key point is that “a person’s vaccine decisions are the result of a complex process” that should be understood as resulting from “a complex process that needs to be understood in its particular context”.
Religion is listed and recognised as a potential factor for vaccine behaviour but may or may not be associated with vaccination status. Larson et al. found that 15.4% of respondents to a global survey thought vaccines were incompatible with their religious belief, yet the study also showed that there was not a direct link between a particular faith type and vaccine response.
“It is imperative to consider the impact of religion in light of other factors, such as politics (both national and international), history (e.g. colonialism), and cultural values (e.g. gender roles).”
Therefore, the relationship between religion and vaccine hesitancy is “complex and context specific”. Hoping to “shed light” on the role of religion in influencing vaccine decisions in practice, the article claims to offer a “complete and coherent typology of religious vaccine scepticism (RVS), based on a literature review.
“RVS here denotes an attitude of doubt or disbelief towards vaccines that originates in, is related to, or is explained as religion.”
Literature review
The typology was developed on a literature review of research into religion’s influence on vaccine decisions. This review included peer-reviewed articles, written in English, across different fields and kinds. Sometimes religion was not the primary focus, but findings involved “significant religious arguments against vaccination”. With the goal of identifying as many arguments as possible, the review was “broad” and “paid equal attention both to frequently mentioned and to rare objections”.
The types were structured according to the “essence of what is considered problematic with vaccines” in the eyes of a religious individual or group in answer to the question “what is the problem with vaccines?” The essence of each type may “span across different religious traditions and groups” because the types encompass elements that are not specific.
The types
Vaccines as irrelevant or destructive
The first type is the “worldview clash” type, in which the “causal explanations of life, health, and disease make vaccination inappropriate as a health intervention”. Considering certain premises, vaccination is “irrational” because it is either “unnecessary” or brings about “negative consequences”.
For example, Trangerud states that members of Christian Science “may not only reject vaccines” but other medical interventions due to a belief that “diseases are illusions” and “only the realisation of this can bring about healing”. In this worldview, human beings are the image of a spiritual God and cannot be sick, a material phenomenon. Furthermore, sin, ignorance of God, or fear (such as that of disease), may cause disease. The appropriate remedy would be prayer and the “correct mindset”.
Another example of a worldview clash type is the perception of polio by the Hausa communities in northern Nigeria, for whom polio (or cutar shan-Inna) is a result of a powerful spirit drinking the blood of a victim’s limb. Healing can be achieved through offering the spirit whatever she informs the traditional healer that she wants, such as food, accompanied by prayer, incense, and herbal massage. Healing occurs when the spirit is satisfied. Thus, the oral polio vaccine “makes very little sense”.
Vaccines interfering with God’s will or revealing distrust
Trangerud indicates that, as with the first type, this second type is “rooted in the premises of a particular worldview”. However, in this type, the role of human beings is not active, as in the first.
“The divine will type describes the passive acceptance of an outcome that is believed to be decided by God, be it health or disease, life or death.”
As an example, Trangerud identifies orthodox Protestants in the Netherlands, whose decisions to accept or reject vaccines are “often” based on religious arguments. Members believe that one shouldn’t, and indeed can’t, interfere with divine providence.
The divine will type is “three-pronged”, involving belief in:
God’s protection from disease
God’s sending of disease
God’s help during disease
Evidently, argues Trangerud, trust is key, but for some “fear might be the other side of the coin”. This could be fear of displaying distrust or of making a bad decision, she suggests. If disease is God’s will, doing nothing and “leaving the outcome to God” might be a “safer alternative” to intervening with vaccination. This type therefore represents a form of “passive or classic fatalism”, the belief that “something will occur regardless of one’s intention or behaviour”. People who hold these views are “generally less compliant with expert advice”.
Passive fatalism is contrasted to active fatalism, which involves both acceptance and active attempts to influence the outcome. Here Trangerud presents the case that “most Muslims” believing diseases occur by God’s will, yet studies suggest this is not an obstacle to seeking medical interventions. Instead, Muslims might accept vaccines as “part of their duty to protect their health”.
Vaccines as unethical
The RVS of the third type relates to issues that are considered “ethically problematic”, and does not apply to all vaccines in general, but certain vaccines. The value judgement of these vaccines relates either to the production of the vaccine (cause-related subtype) or the use of the vaccine (effect-related subtype).
The cause-related subtype describes scepticism towards vaccines “deemed unethical because their production somehow is related to the illicit killing or suffering of a being”. Trangerud’s example is of the cell lines from voluntarily aborted foetuses used to grow viruses, point for rejection for Catholics or other Christians who strongly oppose abortion. Another example is the use of bovine ingredients like foetal bovine serum, identified as a potential concern to Hindus to whom cows are sacred. This is “underresearched in the context of vaccines”, but for drugs and medical products studies have identified a “reluctance” in Hindus.
The effect-related subtype involves scepticism towards vaccines that are found “ethically unacceptable” because they are perceived as encouraging “sexually immoral behaviour”. This association between vaccines and sexual behaviour can be traced to vaccines preventing diseases transmitted through sexual intercourse (human papillomavirus and hepatitis B). Parents may reject these vaccines for their children in favour of the principle of abstinence set down for Christians, Jews, and Muslims, or so studies suggest. Furthermore, some parents fear these vaccines can themselves “trigger early sexual debut or promiscuous behaviour”. Finally, the fear of social stigma if one is “perceived to need such vaccines” may cause hesitancy in cultures where sexual abstinence before marriage is the norm.
Vaccines as defiling the human body
The RVS of the fourth type is based on the idea that “some vaccine ingredients are religiously impure”, either by nature or preparation. They can therefore “defile the human body”. This notion of impurity is different to that of immorality. The impurity type “rejects vaccines because of ingredients that, according to a divine order, are defined as unclean or harmful in essence”.
The example that Trangerud offers is that of pigs, regarded as unclean by Muslims, Jews, and some Christians. Studies have demonstrated that, “to many Muslims”, porcine ingredients are “major concerns and barriers to immunisation”. This can only be overcome by halal certification or proof that the vaccine does not contain prohibited ingredients. Some Islamic leaders and medical experts have declared gelatine to be permissible, having become clean through a process of transformation, but not all scholars accept this.
Porcine ingredients were a problem illustrated by a drop in vaccination coverage in Indonesia after the Indonesian Ulama Council said the new measles-rubella vaccine in 2017 was forbidden by Islamic law. By contrast to other religious groups, some Christians, who “have no problems with eating different types of meat and using other animal products”, hold the belief that the body will be “polluted” if vaccine ingredients from the same animals, alongside chemicals, are injected.
Vaccines as a means of harm
The final RVS is a type “rooted in conspiracy beliefs” that associate vaccines with a plot for “extensive, negative consequences”. These beliefs “need not be related to religion”, but as an RVS type pertain to vaccine conspiracies that target a religious group or community. Some of these conspiracies involve population control through fertility reduction or deadly diseases, with vaccines functioning as “vectors or camouflage for a secret, harmful substance”. Therefore, vaccination threatens both the existence of individuals and their whole community.
“While some people deliberately spread conspiracy rumours to achieve other goals, ordinary people may genuinely believe in the, and be struck with fear or anger.”
The occasional engagement by trusted religious authorities lends credibility to these rumours. This is a complex type, demonstrated by the boycott of the oral polio vaccine by some of the Muslim-majority states in northern Nigeria in 2003. This may appear a “classic religious conspiracy theory” driven by local political and religious leaders, warning that the vaccine had been deliberately contaminated with anti-fertility agents or HIV viruses as part of a plot to reduce Muslim populations. However, later analyses show that the accusations were “only a small piece” of a “larger and much more complex political picture” comprising years of national struggle for political power between the Christian and Muslim regions, poor health infrastructure and differing priorities, previous negative experiences with Western colonialism, racial prejudices, and a vaccine scandal from 1996.
Another aspect of the conspiracy type includes the linking of conspiracy beliefs to a religious narrative. For example, some Christians rejected the COVID-19 vaccine because “they feared it might contain microchips and hence represent ‘the mark of the beast’”. This biblical phrase is associated with end times events, such as persecution of Christians.
Trangerud’s conclusions
“For policymakers and public health workers, it is imperative to know when the solutions to counter vaccine hesitancy are found outside religion.”
Trangerud suggests that the benefits of this study include knowing that RVS is “not necessarily reflected in the canonical doctrines of a religious institution”. While there are examples of teachings that prohibit immunisation, “most religious groups do not have straightforward teachings on the matter”. However, religious doctrines still inform vaccine decision-making. Often, one doctrine is interpreted differently by different groups, such as the case of the religious duty to “preserve life”. Thus, the same doctrine “may be relied on by both acceptors and rejectors of a vaccine”.
The typology that Trangerud offers is based on research that identifies how RVS affects vaccine decisions “on a practical level”. It is useful for those who want to understand the effect of religion on vaccine hesitancy and can help match types to interventions:
For the worldview clash type, the solution may be found within the worldview in question – following the rules of logic laid down by the applicable premises.
For the divine will type, the solution could be to aid believes from passive fatalism to active fatalism, encouraging active participation in caring for one’s health at the same time as respectfully preserving belief in providence or other external forces.
For the immorality and impurity types, some believes may be convinced by arguments or the provision of vaccines with alternative ingredients.
For the conspiracy type, the building of trust is key. The roots of the beliefs must be identified and dealt with individually. Some religious arguments might be helpful.
If you consider yourself religious, are there any aspects of the typology that strike you as interesting or surprising? Have you had to overcome, whether personally or professionally, any of these types? What do you think this paper contributes to the vaccine hesitancy space?
In July 2023 UNAIDS released a report outlining a “clear path” to end AIDS and prepare for and tackle future pandemics in line with Sustainable Development Goals. This report, The Path that Ends AIDS presents data and case studies to highlight the political and financial choices that are critical to achieving “extraordinary” results.
Although the report gives readers reasons to celebrate remarkable progress, it also highlights that AIDS claimed a life every minute in 2022. Approximately 9.2 million people still do not have access to treatment, a number that includes 660,000 children. Women and girls are “disproportionately affected”, especially in sub-Saharan Africa. A statement from UNAIDS indicates that 4,000 women and girls became infected with HIV every week in 2022, but only 42% of districts with HIV incidence over 0.3% in sub-Saharan Africa currently offer dedicated HIV prevention programmes for adolescent girls and young women.
Facts and figures
In 2022 an estimated:
39 million people globally were living with HIV
29.8 million people were accessing antiretroviral therapy
1.3 million people became newly infected with HIV
630, 000 people died from AIDS-related illnesses
95-95-95 targets in sight
A chosen indicator of success within the report is the “95-95-95″ target:
95% of people who are living with HIV know their status
95% of people who know they are living with HIV are on lifesaving antiretroviral treatment
95% of people who are on treatment are virally suppressed
Botswana, Eswatini, Rwanda, the United Republic of Tanzania, and Zimbabwe have already achieved these targets, with a further 16 countries close to doing so; 8 of these countries are in sub-Saharan Africa, the region that accounts for 65% of all people living with HIV.
Politics can promote progress
The report outlines that HIV successes are anchored in strong political leadership, which, according to a UNAIDS statement follows “data, science, and evidence”. Furthermore, this strong leadership identifies and tackles inequalities, engages with communities and organisations, and ensures “sufficient and sustainable funding”.
Winnie Byanyima, Executive Director of UNAIDS, described the end of AIDS as an “opportunity for a uniquely powerful legacy for today’s leaders”.
“They could be remembered by future generations as those who put a stop to the world’s deadliest pandemic. They could save millions of lives and protect the health of everyone. They could show what leadership can do.”
UNAIDS states that progress has been strongest in areas with the “most financial investments”. For example, in eastern and southern Africa new HIV infections have been reduced by 57% since 2010. Increased political will and investment must address key areas such as evidence-based HIV prevention and treatment, health systems integration, non-discriminatory laws, gender equality, and empowered community networks.
“We are hopeful, but it is not the relaxed optimism that might come if all was heading as it should be. It is, instead, a hope rooted in seeing the opportunity for success, an opportunity that is dependent on action.”
Ms Byanyima was emphatic in her call to action: “the way is clear”.
“The facts and figures shared in this report do not show that as a world we are already on the path, they show that we can be.”
Working for children
With the goal of ending AIDS among children, support and investment has contributed to the increase in pregnant or breastfeeding parents living with HIV who access antiretroviral treatment, from 46% in 2010 to 82% in 2022. This has contributed to a 58% reduction in new HIV infections among children, which UNAIDS emphasises is the lowest number since the 1980s.
Protecting human rights
A key paving stone in the pathway of progress has been ensuring that frameworks “enable and protect” human rights. For example, several countries removed harmful laws over the past year, including 5 that have decriminalised same-sex sexual relations.The statement suggests that infection rises are due primarily to a lack of prevention services for “marginalised and key populations” and the barriers presented by “punitive laws and social discrimination”.
In an article for International Affairs in June 2023 Dr Andreas Papamichail of the Centre for Public Health and Policy explores the importance of health policy in addressing “deep-rooted racial inequities”. Dr Papamichail draws on theories of racial capitalism in suggesting that to prepare for future disease outbreaks we must identify and respond to these inequities in our experience of the COVID-19 pandemic. Here we examine the role of vaccine production and distribution, but we encourage readers to access the full article if interested.
Nothing new to see here
Dr Papamichail acknowledges that the “highly inequitable global distribution of vaccines” of the pandemic is “not a new phenomenon”. This is demonstrated by the global experience of diseases like HIV/AIDS. Indeed, during the COVID-19 pandemic as mpox spread internationally beyond its conventionally endemic regions, it became apparent that we had failed to learn from history.
However, Dr Papamichail suggests that there was “initial optimism” for “new policy space” and subsequent changes to international IP laws. For example, the COVIAX initiative, established in March 2020, promised to encourage equity. Alas, this hope was short lived for many as this effort has since been described as a “failure” or “useless”. Furthermore, it “served to entrench precisely the global structures it was supposedly aimed at counteracting”.
“Rather than prevent states who signed up for the initiative from circumventing it and striking bilateral deals with pharmaceutical companies, COVAX in fact enabled these as a concession to get wealthier countries to join the initiative.”
The article contrasts “staggering inequities” with the profit margins of key vaccine producers in evidence of what some describe as “vaccine apartheid”.
“No one is safe until everyone is safe”
The COVID-19 pandemic was host to a range of rhetorical exercises, but Dr Papamichail suggests that one in particular “rings hollow”: “no one is safe until everyone is safe”. He suggests that some of the organisations contributing to this narrative are “deeply embedded and invested in the perpetuation of the system that enables this vaccine apartheid”.
The article explores three dynamics that contribute to racialised inequity:
“The obvious inequity created by the profit incentives of pharmaceutical companies which shape the prioritisation of health issues and the distribution of life-saving vaccines and medicines according to the profitability rather than harm, and the ways in which the global IP regime entrenches these inequities.”
“The consequences of the maldistribution of medical products and technologies are obviously racialised, implying that racial differentiation is a necessary condition for acquiescence to such a brazenly inequitable system.”
“The way in which acts of charity like those emblematised by COVAX become the only possible exception to the legacies of exclusion entrenched by global IP regimes.”
What can we do?
Dr Papamichail suggests that the three dynamics of the COVID-19 pandemic “laid bare multiple interlocking and co-constituting processes”. He emphasises that “domestic and global hierarchies” create “surplus subjects and stratified layers of expendability”, giving the example of the “exposure of the racialised ‘essential worker’ to illness and death”.
“The combined dynamics of expendability, exclusion and inclusion, and maldistribution, which have characterised the pandemic are emblematic of the workings of global racial capitalism, given that they arise out of a system that privileges some forms of labour, some forms of movement, and certain parts of the world over others.”
The conclusion demands greater analysis of race and racism in scholarship on the “intersections between global health and international politics”. Fortunately, Dr Papamichail states that the “sheer scale of inequity” and its pandemic prominence might create “challenges and resistance”.
“Decolonising is not just about reading lists, methods and sites of research, or discourses of global health, but about the material structures (of racial capitalism) that uphold global hierarchies of worth.”
Some “concrete actions” are offered to policymakers and activists, and the most pertinent to vaccines is the call to “challenge” the idea that “IP protections are legitimate” in the light of public funding being able to “de-risk investment”.
Do you agree with the issues raised and this emphasis on IP regimes? Let us know your thoughts on the article if you read it here, and don’t forget to subscribe to get more vaccine updates!
Researchers at 19 institutions comprising the TBVAC-HORIZON have been awarded €9 million in funding to encourage research and development into tuberculosis. This project will specifically consider lung immunity and how infection evades the immune response. The project is coordinated by the Tuberculosis Vaccine Initiative (TBVI) and is expected to last for 4 years.
Why TB?
TB is a bacterial infection spread through droplets expelled from the lungs of an infected person. It mainly targets the lungs and continues to be one of the world’s most devastating infectious diseases. The WHO reports that a total of 1.6 million people died from TB in 2021, which includes 187,000 people with HIV. It is the 13th leading cause of death and follows COVID-19 as the second leading infectious killer.
Although up to 74 million lives were saved through diagnosis and treatment between 2000 and 2021, around $13 billion is needed every year for prevention, diagnosis, treatment, and care to achieve the global target agreed at the 2018 high-level meeting on TB. Ending the TB epidemic by 2030 is a health target of the Sustainable Development Goals (SDGs).
Currently there is only for effective vaccine for TB, which is usually given to infants and young children, as it is less effective for adults. Therefore, development of improved vaccines is a priority for the WHO.
TBVAC-HORIZON
Although there are a few candidates in clinical trials, the pipeline requires innovation. The programme will aim to address this need by examining the immune responses to infection in the lung, identifying biomarkers to “rationalise vaccine design” and improve vaccine immunity monitoring. Researchers within the programme will compare candidate vaccines and establish novel delivery systems and adjuvant formulations. A novel GMP platform for live attenuated vaccines will also be developed.
Centre National de la Recherche Scientifique (CNRS)
Université Toulouse III – Paul Sabatier (UT3)
Istituto Nazionale per le Malattie Infettive ‘Lazzaro Spallanzani’ (INMI-IRCCS)
Institut Pasteur (IP)
Institut Pasteur de Lille (IPL)
Leiden University Medical Centre (LUMC)
Statens Serum Institut (SSI)
University of Zaragoza (UNIZAR)
University of Ulm (UULM)
CZ Vaccines, S.A. (CZV)
University of Basel (UNIBAS)
Vaccine Formulation Institute CH, Ltd. (VFI)
Department of Health (UKHSA)
London School of Hygiene and Tropical Medicine (LSHTM)
Medicines and Healthcare Products Regulatory Agency (MHRA)
University of Leicester (ULEIC)
University of Oxford (UOXF)
Professor Andrea Cooper from the University of Leicester’s Tuberculosis Research Group (LTBRG) is one of the lead scientists for the project. She hopes that by “combining forces” and “identifying biomarkers” they can “improve vaccines as well as improving monitoring of vaccine immunity”.
“The LTBRG already brings together scientists and academic clinicians to focus on overcoming tuberculosis at a local and national level, but this project will bring expertise from across Europe together to advance our research even further.”
University of Oxford’s Professor Helen McShane is “enormously excited about the science we plan to perform”. As PI Translational Research Professor McShane is looking forward to covering “basic and translational science with an interdisciplinary and integrated approach”.
“This work will advance understanding of protective immunity, particularly in the target organ, the lung, and in parallel improve the development of novel TB vaccine candidates.”
Like many other consortia led by TBVI, partners will collaborate on “excellent science” to secure Europe’s “leading role” in the “development of a more effective TB vaccine”.
To stay in the loop on vaccines for TB and other infectious diseases don’t forget to subscribe.
In June 2023 the WHO and the Global Fund to Fight AIDS, Tuberculosis, and Malaria (the Global Fund) committed to a revised Strategic Framework for Collaboration. This is designed to build “stronger and more resilient health systems” and encourage collaboration with positive effects at country, regional, and global level. It is a five-year framework that builds on a previous agreement, signed in 2018. It also aligns with the Global Fund Strategy and the WHO General Programme of Work, which “put communities at the centre of the health response” and address pandemic preparedness and climate change challenges.
Fighting AIDS, TB, and malaria
Dr Tedros Adhanom Ghebreyesus, WHO Director-General. Remarked that “health budgets globally are strained and under pressure”.
“It is imperative for our two organisations to continue to work together to support countries to expand access to services for the three diseases as part of their journey towards universal health coverage.”
He admitted that we have seen “slowing progress” towards ending the epidemics of these diseases, which, coupled with “emerging health challenges”, requires “stronger collaboration” than ever.
Health systems under pressure
Peter Sands, Executive Director of the Global Fund, agreed that this partnership is “more critical than ever” due to “interlocking and intersecting crises”.
“Crises shock global systems and roll back gains, with the world’s most vulnerable people bearing the brunt. Organisations like ours are most effective when we collaborate closely with national governments and other trusted partners to strengthen local, community-driven systems for health.”
Achievements so far
Although progress has slowed, WHO and the Global Fund recognise “significant achievements at country level”:
20 countries are now implementing, in a more efficient and cost-effective way, differentiated service delivery for HIV testing, treatment, advanced HIV disease care, as well as virtual interventions to reach those unaware of their HIV status.
Collaboration has enabled early guidance and surveys on dual testing for COVID-19 and TB, allowing for improved detection of people with TB through the innovations adopted during and after the COVID-19 emergency.
Strategic initiatives on malaria enabled accelerated progress towards malaria elimination. Since 2018, eight countries have been certified malaria-free by WHO, with five more preparing for certification in 2023 and 2024.
The partnership also provides the foundation to accelerate the implementation of innovative approaches, such as the new WHO Insecticide Treated Nets Guidelines for malaria and the scale-up of new-shorter treatments for multidrug-resistant TB.
Valuable support was provided in the development of 50 evidence-based and costed national strategic plans aligned to the latest WHO guidelines, serving as a basis for high-quality funding requests to the Global Fund.
WHO’s work to track health expenditure in 59 low- and middle-income countries has informed national health policy. Joint work to support cross-programme efficiency analysis in 13 countries has reduced fragmentation and duplication.
More work to do
Despite these achievements, work is left to “accelerate progress” towards ending AIDS, TB, and malaria epidemics and to “build strong health systems that are also capable of responding to the next emergency”.
The new framework divides the 35 areas for collaboration into 4 categories:
Health policies and normative guidance
Advocacy and health governance
Health products and innovations
Technical support and capacity building
For more health updates like this, make sure you subscribe to our weekly newsletter here.
Our next interview is with Dr Jay Berzofsky, Chief of the Vaccine Branch at NCI’s Centre for Cancer Research. He joined us at the Congress to participate in the Cancer and Immunotherapy Vaccines track, during which he explored triple synergistic combination immunotherapy. We are so grateful for Dr Berzofsky’s time and insights into cancer vaccine development and the challenges that come with it. We hope you enjoy the interview!
Introducing Dr Berzofsky
Dr Berzofsky kindly explains a bit about how his role works within the programme.
“We are government employees…we have nothing to do with grants for universities and so forth, but we do our own research.”
The branch is the vaccine branch, and they work on “basic science” and its applications to vaccines for HIV, cancer, and viruses that cause cancer, as well as COVID-19.
Triple synergistic combination immunotherapy
Dr Berzofsky kindly gave us a preview of his session the following day, which was to explore triple synergistic combination immunotherapy. He began by explaining that “there are different reasons why certain cancers may not respond well to immunotherapy”. He introduces “hot tumours”, those that are “inflamed” with T cells that “could kill the tumour cells”. However, the “tumour microenvironment” is “very immunosuppressive” and “prevents them from doing their job”.
“The T cells are there, but they need to be enabled.”
Next, Dr Berzofsky discusses “cold tumours”. These have no T cells infiltrating, often because the tumour doesn’t induce a good immune response. Essentially, the “immune system doesn’t see it as foreign”. These two different kinds of tumours need different strategies, suggests Dr Berzofsky.
“In the case of a hot tumour, you want to block the immunosuppression, to allow the T cells that are there to work.”
This is the case for melanoma, lung cancer, and a “number of other cancers”.
“In cold tumours, you need to generate an immune response, and that’s where the vaccine can come in.”
Inducing a T cell response that the “tumour itself failed to induce” converts the tumour from a cold tumour to a hot tumour. The vaccine, and the blockers of “negative regulation” such as checkpoint inhibitors, are synergistic!
“The vaccine can induce the T cells, but they won’t work if you don’t block the immunosuppressive environment.”
Initial challenges
Clearly developing therapeutic cancer vaccines is a challenging task. When we asked Dr Berzofsky about this, he reckoned that “there are a number of challenges!” A major challenge that he does discuss is the need to encourage the immune system to “reject” the cancer as it might a transplant. The immune system can be “exquisitely specific”, unlike an external approach like chemotherapy; it can “distinguish very cleanly” what is foreign in the body.
“But remember, the cancer cells are not foreign organisms like bacteria or viruses that are completely different from your own cells – they arose from your own cells.”
The target therefore, is a vaccine that can “train the immune system to see those unique differences”.
Further challenges
Another challenge that Dr Berzofsky identifies is that there are “many immunosuppressive mechanisms” beyond checkpoints.
“One has this panoply of suppressive mechanisms to overcome.”
We don’t have “really good ways” of overcoming these in humans yet, so Dr Berzofsky calls for research to “more effectively illuminate these other suppressive mechanisms”.
“It may be a daunting task to try to block 8 or 10 different suppressive mechanisms at the same time…so we need to find common nodes of intersection where some of these suppressive mechanisms interact, so we can block more than one at the same time.”
What more can be done?
As Dr Berzofsky has suggested, more work can be done, as always! We asked about potential areas for development that he can identify. Following from his previous answer, he emphasises the importance of finding “better ways, that are safe, to eliminate these immunoregulatory cells”. However, we also have to “strike the right balance”; they are there for a reason.
“It’s just going to take more research.”
Although we can make progress in animals, Dr Berzofsky suggests that the next step is “human clinical trials”.
Coming to the Congress
When we asked Dr Berzofsky about why he was joining us, he commented on the quality of his colleagues’ presentations!
“Hearing all the wonderful speakers that come to this meeting every year!”
Apart from the opportunity to learn, Dr Berzofsky was looking forward to meeting and developing potential collaborations.
“One of the things that’s important in science as in so many fields, is networking, because none of us can do everything in our own small laboratory.”
We are so grateful to Dr Berzofsky for his time and insights into some of the most challenging vaccine endeavours of our time. We hope to continue this conversation at future events. For more like this, make sure you subscribe to our weekly newsletters.
Just days after the COVID-19 pandemic was declared no longer a public health emergency of international concern (PHEIC), mpox has followed suit. Cases of mpox, formerly monkeypox, have declined since the previous meeting of the IHR Emergency Committee. Despite this positive declaration, the Committee acknowledges “remaining uncertainties about the disease”, relating to “modes of transmission”, “poor quality of some reported data”, and “continued lack of effective countermeasures in the African countries” where mpox “occurs regularly”.
Updates on the situation
The Director-General, Dr Tedros Adhanom Ghebreyesus, commented on the sustained decline of cases across the world. He noted that almost 90% fewer cases have been reported over 3 months compared to the previous 3 months. However, the virus is still transmitting in certain communities.
At the meeting, representatives of Japan, Nigeria, and the UK provided updates on the situation within their countries. The Secretariat offered a “comprehensive update” on the epidemiological situation and response efforts, with a further update from the WHO Region of Africa. The Region reported that the majority of the 1500+ confirmed cases since January 2022 have been in Nigeria and the Democratic Republic of the Congo.
“There was little information on modes of transmission and the quality of reported data through surveillance systems was uneven in the African Region.”
The current global risk is described as “moderate” across much of the globe.
Knowledge gaps
Although progress has been made through a global effort, the Committee recognised “remaining concerns”, which include duration of immunity after infection or vaccination, “insufficient evidence about vaccine effectiveness”, and “poor quality of data and inconsistency in reporting of cases”.
Despite concerns about the potential effects of large social gatherings among “high-risk groups” it was noted that many gatherings took place last year without a spoke in case numbers. Furthermore, some regions have post-emergency plans and have started to integrate the response into sexually transmissible infection programmes.
In Africa there are “concerns” about the situation, particularly concerning “recurring zoonotic transmission”. Wider concerns were raised about lack of access to vaccines, medicines, and diagnostic testing in many LMICS.
“Not all countries are receiving the support they need or have structures or systems to response to mpox, including inadequate support for marginalised groups.”
Moving to a long-term strategy
Although the Committee acknowledges the “uncertainties” surrounding mpox, it encourages a transition to a “long-term strategy” instead of the emergency measures demanded in a PHEIC. WHO states that the Committee “emphasised the necessity for long-term partnerships” to “mobilise” the necessary support for “sustaining surveillance, control measures and research for the long-term elimination of human-to-human transmission”, and “mitigation of zoonotic transmissions”.
“Integration of mpox prevention, preparedness, and response within national surveillance and control programmes, including for HIV and other sexually transmissible infections, was reiterated as an important element of this longer-term transition.”
The Committee noted that progress has been made “largely in the absence of outside funding support”. Furthermore, “longer-term control and elimination” will be unattainable without such support.
Temporary Recommendations
Just as with the COVID-19 change last week, the WHO Director-General issued Temporary Recommendations relating to the outbreak. These are intended to meet the objectives to “interrupt human-to-human transmission, protect the vulnerable, and minimise zoonotic transmission”.
“In implementing these Temporary Recommendations, States Parties should ensure full respect for the dignity, human rights, and fundamental freedoms of persons.”
Sustain and promote key elements of the mpox response strategy and review experience to inform public health policies, programmes, and actions.
Develop and implement integrated mpox control plans and an elimination strategy with the aim of preventing and stopping human-to-human transmission and/or mitigating zoonotic transmissions.
Maintain epidemiological surveillance of mpox, making every effort to ensure laboratory confirmation of suspected cases and reporting to WHO of confirmed cases and probable cases.
Report immediately all confirmed travel-related mpox cases to WHO.
Integrate mpox detection, prevention, care, and research with existing and innovative HIV and sexually transmitted disease prevention and control programmes, and other health services as appropriate.
Sustain and invest in risk communication and community support and engagement for affected communities and at-risk groups, including through health authorities and civil society.
Continue to implement interventions to avoid stigma and discrimination against any individuals or group that may be affected by mpox.
Support and enhance access to diagnostics, vaccines, and therapeutics to advance global health equity, in particular for most affected communities worldwide, including gay, bisexual, and other men who have sex with men, with special attention to those most marginalised within those groups, and in resource-constrained countries where mpox is endemic.
Continue to strengthen diagnositc capacity, decentralised access to testing and genomic sequencing, including sharing of genetic sequence data through public databases.
Continue to make vaccines available for primary preventative (pre-exposure) and post-exposure vaccination for persons and communities at high risk of mpox.
Ensure provision of optimal clinical care with infection prevention and control measures in place for suspected or confirmed mpox in all clinical settings. Ensure training of health care providers accordingly.
Strengthen capacity in resource-limited and rural settings where mpox continues to occur, to better understand modes of transmission, quantify resource needs, and respond to outbreaks and sustained chains of transmission.
Implement a coordinated research agenda to generate and promptly disseminate evidence for key scientific, social, clinical, and public health aspects of mpox prevention and control. Continue clinical trials of medical countermeasures, including vaccines, therapeutics, and diagnostics, in different populations, in addition to monitoring of vaccine safety, effectiveness, and duration of protection from infection and vaccination.
Countries in West, Central, and East Africa, where mpox is endemic should make additional efforts to elucidate mpox-related risk, vulnerability, and impact, and to investigate, understand, and control mpox in their respective settings, including the consideration of zoonotic, sexual, and other modes of transmission in different demographic groups.